-
Sexuality After Spinal Cord Injury
Wikipedia
The ability to experience sexual pleasure and orgasm are among the top priorities for sexual rehabilitation among injured people. [14] Much research has been done into erection . [14] By two years post-injury, 80% of men recover at least partial erectile function, [15] though many experience problems with the reliability and duration of their erections if they do not use interventions to enhance them. [16] Studies have found that half [15] or up to 65% of men with SCI have orgasms, [17] although the experience may feel different than it did before the injury. [15] Most men say it feels weaker, and takes longer and more stimulation to achieve. [18] Common problems women experience post-SCI are pain with intercourse and difficulty achieving orgasm. [19] Around half of women with SCI are able to reach orgasm, usually when their genitals are stimulated. [20] Some women report the sensation of orgasm to be the same as before the injury, and others say the sensation is reduced. [5] Complete and incomplete injury [ edit ] The severity of the injury is an important aspect in determining how much sexual function returns as a person recovers. [15] [21] According to the American Spinal Injury Association grading scale, an incomplete SCI is one in which some amount of sensation or motor function is preserved in the rectum . [10] This indicates that the brain can still send and receive some messages to the lowest parts of the spinal cord, beyond the damaged area. ... Although erections are not necessary for satisfying sexual encounters, many men see them as important, and treating erectile dysfunction improves their relationships and quality of life. [78] Whatever treatment is used, it works best in combination with talk-oriented therapy to help integrate it into the sex life. [65] Oral medications and mechanical devices are the first choice in treatment because they are less invasive, [79] are often effective, and are well tolerated. [80] Oral medications include sildenafil (Viagra), tadalafil (Cialis), and vardenafil (Levitra). [81] [65] Penis pumps induce erections without the need for drugs or invasive treatments. To use a pump, the man inserts his penis into a cylinder, then pumps it to create a vacuum which draws blood into the penis, making it erect. [82] [65] He then slides a ring from the outside of the cylinder onto the base of the penis to hold the blood in and maintain the erection. [82] [53] A man who is able to get an erection but has trouble maintaining it for long enough can use a ring by itself. [63] [83] The ring cannot be left on for more than 30 minutes and cannot be used at the same time as anticoagulant medications. [53] If oral medications and mechanical treatments fail, the second choice is local injections: [79] medications such as papaverine and prostaglandin that alter the blood flow and trigger erection are injected into the penis. [84] This method is preferred for its effectiveness, but can cause pain and scarring. [85] Another option is to insert a small pellet of medication into the urethra , but this requires higher doses than injections and may not be as effective. [85] Topical medications to dilate the blood vessels have been used, but are not very effective or well tolerated. [80] Electrical stimulation of efferent nerves at the S2 level can be used to trigger an erection that lasts as long as the stimulation does. [86] Surgical implants, either of flexible rods or inflatable tubes, are reserved for when other methods fail because of the potential for serious complications, which occur in as many as 10% of cases. [80] They carry the risk of eroding penile tissue (breaking through the skin). [87] Although satisfaction among men who use them is high, if they do need to be removed implants make other methods such as injections and vacuum devices unusable due to tissue damage. [80] It is also possible for erectile dysfunction to exist not as a direct result of SCI but due to factors such as major depression, diabetes , or drugs such as those taken for spasticity. [88] Finding and treating the root cause may alleviate the problem. For example, men who experience erectile problems as the result of a testosterone deficiency can receive androgen replacement therapy . [44] Ejaculation and male fertility [ edit ] Without medical intervention, the male fertility rate after SCI is 5–14%, but the rate increases with treatments. [89] Even with all available medical interventions, fewer than half of men with SCI can father children. [90] Assisted insemination is usually required. [91] As with erection, therapies used to treat infertility in uninjured men are used for those with SCI. [65] For anejaculation in SCI, the first-line method for sperm retrieval is penile vibratory stimulation (PVS). [8] [81] [92] [93] A high-speed vibrator is applied to the glans penis to trigger a reflex that causes ejaculation, usually within a few minutes. [92] Reports of efficacy with PVS range from 15 to 88%, possibly due to differences in vibrator settings and experience of clinicians, as well as level and completeness of injury. [92] Complete lesions strictly above Onuf's nucleus (S2–S4) are responsive to PVS in 98%, but complete lesions of the S2–S4 segments are not. [8] In case of failure with PVS, spermatozoa are sometimes collected by electroejaculation : [8] [92] [93] an electrical probe is inserted into the rectum, where it triggers ejaculation. [81] The success rate is 80–100%, but the technique requires anaesthesia and does not have the potential to be done at home that PVS has. [21] Both PVS and electroejaculation carry a risk of autonomic dysreflexia, so drugs to prevent the condition can be given in advance and blood pressure is monitored throughout the procedures for those who are susceptible. [94] Massage of the prostate gland and seminal vesicles is another method to retrieve stored sperm. [65] [92] If these methods fail to cause ejaculation or do not yield sufficient usable sperm, sperm can be surgically removed by testicular sperm extraction [21] or percutaneous epididymal sperm aspiration . [8] These procedures yield sperm in 86–100% of cases, but nonsurgical treatments are preferred. [21] Premature or spontaneous ejaculation is treated with antidepressants including selective serotonin reuptake inhibitors , which are known to delay ejaculation as a side effect . [63] Women [ edit ] Compared with the options available for treating sexual dysfunction in men (for whom results are concretely observable), those available for women are limited. [95] For example, PDE5 inhibitors , oral medications for treating erectile dysfunction in men, have been tested for their ability to increase sexual responses such as arousal and orgasm in women—but no controlled trials have been done in women with SCI, and trials in other women yielded only inconclusive results. [96] In theory, women's sexual response could be improved using a vacuum device made to draw blood into the clitoris, but few studies on treatments for sexual function in women with SCI have been carried out. [83] There is a particular paucity of information outside the area of reproduction. [5] Education and counseling [ edit ] Counseling about sex and sexuality by medical professionals, psychologists , social workers , and nurses is a part of most SCI rehabilitation programs. [70] Education is part of the follow-up treatment for people with SCI, [20] as are psychotherapy , peer mentorship , and social activities; these are helpful for improving skills needed for socializing and relationships. [15] Rather than addressing sexual dysfunction strictly as a physical problem, appropriate sexual rehabilitation care takes into account the individual as a whole, for example addressing issues with relationships and self-esteem. [97] Sexual counseling includes teaching techniques to manage depression and stress, and to increase attention to preserved sensations during sexual activity. [55] Education includes information about birth control or assistive devices such as those for positioning in sex, or advice and ideas for addressing problems such as incontinence and autonomic dysreflexia. [98] Many SCI patients have received misinformation about the effects of their injury on their sexual function and benefit from education about it. [10] Although sexual education shortly after injury is known to be helpful and desired, it is frequently missing in rehabilitation settings; [15] a common complaint from those who go through rehabilitation programs is that they offer insufficient information about sexuality. [57] Longer-term education and counseling on sex after discharge from a hospital setting are especially important, [99] yet sexuality is one of the most often neglected areas in long-term SCI rehabilitation, particularly for women. [61] Care providers may refrain from addressing the topic because they feel intimidated or unequipped to handle it. [11] Clinicians must be circumspect in bringing up sexual matters since people may be uncomfortable with or unready for the subject. [44] Many patients wait for providers to broach the topic even if they do want the information. [57] A person's experience in managing sexuality after the injury relies not only on physical factors like severity and level of the injury, but on aspects of life circumstances and personality such as sexual experience and attitudes about sex. [15] As well as evaluating physical concerns, clinicians must take into account factors that affect each patient's situation: gender, age, cultural, and social factors. [71] Aspects of patients' cultural and religious backgrounds, even if unnoticed before the injury caused sexual dysfunction, affect care and treatments—particularly when cultural attitudes and assumptions of patients and care providers conflict. [100] Health professionals must be sensitive to issues of sexual orientation and gender identity , showing respect and acceptance while communicating, listening, and emotionally supporting. [44] Providers who treat SCI have been found to assume their patients are heterosexual or to exclude LGBTQ patients from their awareness, potentially resulting in substandard care. [101] Academic research on sexuality and disability under-represents LGBTQ perspectives as well. [3] As well as the patient, the partner of an injured person frequently needs support and counseling. [102] It can help with adjustment to a new relationship dynamic and self-image (such as being placed in the role of caretaker) or with stresses that arise in the sexual relationship. [102] Frequently, partners of injured people must contend with feelings like guilt, anger, anxiety, and exhaustion while dealing with the added financial burden of lost wages and medical expenses. [103] Counseling aims to strengthen the relationship by improving communication and trust. [29] Children and adolescents [ edit ] Not only does SCI present children and adolescents with many of the same difficulties adults face, it affects the development of their sexuality. [104] Although substantial research exists on SCI and sexuality in adults, very little exists on the ways in which it affects development of sexuality in young people. [105] Injured children and adolescents need ongoing, age-appropriate sex education that addresses questions of SCI as it relates to sexuality and sexual function. [106] Very young children become aware of their disabilities before their sexuality, but as they age they become curious just as able-bodied children do, and it is appropriate to provide them with increasing amounts of information. [105] Caregivers help the child and family prepare for transition into adulthood, including in sexuality and social interaction, beginning early and intensifying during adolescence. [107] Parents need education about the effects of SCI on sexual function so that they can answer their children's questions. [105] Once patients reach their teens, they need more specific information about pregnancy, birth control, self-esteem, and dating. [77] Teenagers with lost or reduced genital sensation benefit from education about alternative ways to experience pleasure and satisfaction from sexual acts. [108] The teen years are often particularly difficult for those with SCI, in terms of body image and relationships. [109] Given the importance they place on sexuality and privacy, adolescents may experience humiliation when parents or caregivers bathe them or take care of bowel and bladder needs. [110] They can benefit from sexuality counseling, support groups, [109] and mentoring by adults with SCI who can share experiences and lead discussions with peers. [77] With the right care and education from family and professionals, injured children and adolescents can develop into sexually healthy adults. [19] Changes in sexual practices [ edit ] People make a variety of sexual adaptations to help adjust to SCI. ... Intrauterine devices could have dangerous complications that could go undetected if sensation is reduced. [47] [73] Diaphragms that require something to be inserted into the vagina are not usable by people with poor hand function. [126] An option of choice for women is for partners to use condoms . [126] [125] Long-term adjustment [ edit ] In the first months after an injury, people commonly prioritize other aspects of rehabilitation over sexual matters, but in the long term, adjustment to life with SCI necessitates addressing sexuality. [44] Although physical, psychological and emotional factors militate to reduce the frequency of sex after injury, it increases after time. [15] As years go by, the odds that a person will become involved in a sexual relationship increase. [121] Difficulties adjusting to a changed appearance and physical limitations contribute to reduced frequency of sexual acts, and improved body image is associated with an increase. [5] Like frequency, sexual desire and sexual satisfaction often decrease after SCI. [105] The reduction in women's sexual desire and frequency may be in part because they believe they can no longer enjoy sex, or because their independence or social opportunities are reduced. [5] As time goes by people usually adjust sexually, adapting to their changed bodies. [19] Some 80% of women return to being sexually active, [50] and the numbers who report being sexually satisfied range from 40 to 88%. [127] Although women's satisfaction is usually lower than before the injury, [5] it improves as time passes. [29] Women report higher rates of sexual satisfaction than men post-SCI for as many as 10–45 years. [57] More than a quarter of men have substantial problems with adjustment to their post-injury sexual functioning. [128] Sexual satisfaction depends on a host of factors, some more important than the physical function of the genitals: intimacy, quality of relationships, satisfaction of partners, [15] willingness to be sexually experimental, and good communication. [19] Genital function is not as important to men's sexual satisfaction as are their partners' satisfaction and intimacy in their relationships. [70] For women, quality of relationships, closeness with partners, sexual desire, and positive body image, as well as the physical function of the genitals, contribute sexual satisfaction. [129] For both sexes, long-term relationships are associated with higher sexual satisfaction. [15] Relationships [ edit ] A catastrophic injury such as SCI puts strain on marriages and other romantic relationships, which in turn has important implications for quality of life.

-
Restless Legs Syndrome
Wikipedia
Karl Axel Ekbom in 1945. [97] A point of confusion is that RLS and delusional parasitosis are entirely different conditions that have both been called "Ekbom syndrome", as both syndromes were described by the same person, Karl-Axel Ekbom . [98] Today, calling WED/RLS "Ekbom syndrome" is outdated usage, as the unambiguous names (WED or RLS) are preferred for clarity. ... The Journal of Clinical Psychiatry . 75 (7): e679–94. doi : 10.4088/jcp.13r08692 . PMID 25093484 . ^ St. ... Neurotherapeutics (Review). 9 (4): 776–90. doi : 10.1007/s13311-012-0139-4 . ... PMID 22923001 . ^ Neiman, J; Lang, AE; Fornazzari, L; Carlen, PL (May 1990). ... Advanced Peripheral Nerve Surgery and Minimal Invasive Spinal Surgery . Acta Neurochirurgica. 97 . pp. 69–70. doi : 10.1007/3-211-27458-8_15 .BTBD9, MEIS1, PTPRD, TF, POMC, DRD3, MAP2K5, SNCA, PRKN, MFN2, LRRK2, PARK7, FTL, HTRA2, VPS13C, DNAJC6, ATXN7, LINC02086, PINK1, UCHL1, RLS1, CASC16, PODXL, MYT1, LINC02520, LINC01478, CCDC148, SKOR1, HMOX1, TOX3, DRD2, VDR, MAOA, RLS3, CHM, FXYD1, TH, CHMP2B, SLC11A2, ATXN1, HAMP, GABRR3, RLS4, RLS6, NTS, ADH1B, HMOX2, CRP, GABRA4, FXN, EEF1A2, DMRT1, KNG1, IL1B, HFE, MPZ, MAOB, NOS1, ATXN3, ZC4H2, MIXL1, REEP1, AVP, PCDHA3, MOCOS, FAT2, GABRR2, NANS, SLC25A37, ATL1, PYCARD, GCH1, FMR1, C3, TRAPPC6B, CAD, TMPRSS6, DRD4, GLO1, C9orf72, DBP, MIR122, LINC00423, MIR330, RLS2, CPT1B, CHKB, RLS5, KCTD18, NPAS2, SPATS2L, MCF2L, NKX2-1, TFRC, IL17A, TRA, AFP, SLC6A3, SLC1A2, L1CAM, ATXN2, LRP2, TSPAN31, REN, LY6E, SMCP, SERPINA1, TNF, TYMS, IGLC2, SCAF11, CNTN3, HNMT, ZEB2, IGHA1, LITAF, SLC9A3R2, APLN, UTRN, RNMT, GEMIN2, ATRN, FGF23, NR4A3, IGKC, TBP

-
Trichomoniasis
Wikipedia
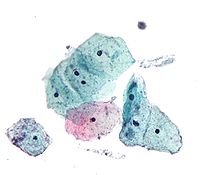
Trichomonas vaginalis culture tests are relatively cheap; however, sensitivity is still somewhat low (70-89%). [20] The third method includes the nucleic acid amplification tests (NAATs) which are more sensitive. [20] These tests are more costly than microscopy and culture, and are highly sensitive (80-90%). [21] Prevention [ edit ] Use of male condoms or female condoms may help prevent the spread of trichomoniasis, [22] although careful studies have never been done that focus on how to prevent this infection. ... The American Journal of Tropical Medicine and Hygiene . 90 (5): 800–804. doi : 10.4269/ajtmh.13-0723 . ... "Trichomoniasis and HIV interactions: a review" . Sexually Transmitted Infections . 89 (6): 426–33. doi : 10.1136/sextrans-2012-051005 . ... Gynekologie (in Czech) (2nd ed.). Prague: Galen. p. 136. ISBN 978-80-7262-501-7 . ^ a b c d Munson E (January 2014). ... Trichomoniasis - CDC Fact Sheet. 2012. ^ Satterwhite CL, Torrone E, Meites E, Dunne EF, Mahajan R, Ocfemia MC, et al. (March 2013).
-
Autoimmune Lymphoproliferative Syndrome
Wikipedia
The increased proliferation of lymphoid cells can cause the size of lymphoid organs such as the lymph nodes and spleen to increase ( lymphadenopathy and splenomegaly , present in respectively over 90% and over 80% of patients). The liver is enlarged ( hepatomegaly ) in 30 - 40% of patients. ... Sirolimus (rapamycin, rapamune) which is a mTOR ( mammalian target of rapamycin ) inhibitor [17] can be active in most patients and can in some cases lead to complete or near-complete resolution of autoimmune disease (>90%) [18] [19] With this treatment most patients have complete resolution of lymphoproliferation, including lymphadenopathy and splenomegaly (>90%) and have elimination of peripheral blood DNTs. ... "The autoimmune lymphoproliferative syndrome: An experiment of nature involving lymphocyte apoptosis" . Immunologic Research . 40 (1): 87–92. doi : 10.1007/s12026-007-8001-1 . ... Journal of Allergy and Clinical Immunology . 125 (4): 946–949.e6. doi : 10.1016/j.jaci.2009.12.983 . ... "Pyrimethamine treatment does not ameliorate lymphoproliferation or autoimmune disease in MRL/lpr-/- mice or in patients with autoimmune lymphoproliferative syndrome". American Journal of Hematology . 82 (12): 1049–55. doi : 10.1002/ajh.21007 .FAS, FASLG, CASP10, NRAS, CASP8, PRKCD, TNFAIP3, RASGRP1, IL10, TRBV20OR9-2, KRAS, SPP1, UNC13D, IL17A, STAT3, FOXP3, B3GAT1, CTLA4, PRF1, CDR3, FADD, TIMP1, TNF, MIR21, EOMES, MIR146A, IL17F, PPIG, LSM2, BCL2L11, TNFRSF13C, KLRG1, TCF7, MMRN1, SMUG1, ADA2, KRT20, LYPLA1, ABCD1, HNF1A, TAP1, AIRE, XIAP, BCL2, CASP9, MS4A1, CD27, CD28, CD48, LRBA, CETN2, COL4A2, MTOR, HLA-A, HMMR, IFNG, IL2RA, ISG20, SH2D1A, PCNA, PIK3CD, APCS, SLC6A3, STAT5B, RN7SL263P
-
Aleutian Disease
Wikipedia
Retrieved 7 April 2008 . ^ Porter DD, Larsen AE, Porter HG (May 1973). "The pathogenesis of Aleutian disease of mink. 3. ... PMID 19961696 . ^ ELIMINATION OF PATHOGENIC INFECTION IN FARMED ANIMAL POPULATIONS ^ Canuti M, O'Leary KE, Hunter BD, Spearman G, Ojkic D, Whitney HG, Lang AS (January 2016).

-
Common Cold
Wikipedia
CMAJ : Canadian Medical Association Journal . 186 (3): 190–99. doi : 10.1503/cmaj.121442 . PMC 3928210 . ... Retrieved 19 March 2013 . ^ a b Eccles p. 80 ^ a b Mourtzoukou EG, Falagas ME (September 2007). ... PMC 7061814 . PMID 25420096 . ^ a b Shefrin AE, Goldman RD (November 2009). "Use of over-the-counter cough and cold medications in children" (PDF) . ... British Journal of Clinical Pharmacology . 82 (5): 1393–98. doi : 10.1111/bcp.13057 . ... PMID 24335668 . ^ Eccles p. 76 ^ a b Eccles p. 90 ^ "The Cost of the Common Cold and Influenza" .SARS1, COPD, SARS2, HGF, LDLR, AQP4, P2RY12, IFIH1, SLC17A5, DUSP10, PLAAT3, ABCB6, SELP, SERPINA1, CTLA4, SLC26A4, NOS2, MYCN, CXCL10, IL13, IL6, ICAM1, GCG, NANOS2

-
Poor Ovarian Reserve
Wikipedia
FSH assays can differ somewhat so reference ranges as to what is normal, premenopausal or menopausal should be based on ranges provided by the laboratory doing the testing. Estradiol (E2) should also be measured as women who ovulate early may have elevated E2 levels above 80 pg/mL (due to early follicle recruitment, possibly due to a low serum inhibin B level) which will mask an elevated FSH level and give a false negative result. [14] High FSH strongly predicts poor IVF response in older women, less so in younger women. ... Kent UK: Anshan. p. 134. ISBN 978-1-904798-96-5 . ^ Navot D, Rosenwaks Z, Margalioth EJ (September 1987). ... Fertil. Steril . 84 (3): 756.e1–756.e3. doi : 10.1016/j.fertnstert.2005.02.049 . ... "Premature ovarian failure and dehydroepiandrosterone". Fertil. Steril . 91 (2): 644–6. doi : 10.1016/j.fertnstert.2007.11.055 . ... "Treatment of autoimmune premature ovarian failure" . Hum. Reprod . 14 (7): 1777–82. doi : 10.1093/humrep/14.7.1777 .
-
Herpes Simplex
Wikipedia
As many as one in seven Canadians aged 14 to 59 may be infected with herpes simplex type 2 virus [85] and more than 90 per cent of them may be unaware of their status, a new study suggests. [86] In the United States, it is estimated that about 1,640,000 HSV-2 seroconversions occur yearly (730,000 men and 910,000 women, or 8.4 per 1,000 persons). [87] In British Columbia in 1999, the seroprevalence of HSV-2 antibody in leftover serum submitted for antenatal testing revealed a prevalence of 17%, ranging from 7% in women 15–19 years old to 28% in those 40–44 years. [88] In Norway, a study published in 2000 found that up to 70–90% of genital initial infections were due to HSV-1. [89] In Nova Scotia, 58% of 1,790 HSV isolates from genital lesion cultures in women were HSV-1; in men, 37% of 468 isolates were HSV-1. [90] History Herpes has been known for at least 2,000 years. ... Dental Clinics of North America . 58 (2): 265–80. doi : 10.1016/j.cden.2013.12.001 . ... Bulletin of the World Health Organization . 86 (10): 805–12, A. doi : 10.2471/blt.07.046128 . ... Aging . 20 (4): 457–65. doi : 10.1016/S0197-4580(99)00055-X . PMID 10604441 . S2CID 23633290 . ^ Pyles RB (2001). ... Dermatol . 41 (6): 996–1001. doi : 10.1016/S0190-9622(99)70260-4 . PMID 10570387 . ^ Leung DT, Sacks SL (October 2003).NECTIN1, NECTIN2, ACKR1, UBE3B, TP53, ZNF35, IFNA13, IFNG, ERVK-6, APOE, LAT, ERBB2, TLR3, IL2, TNFRSF14, AFP, THBS1, GLB1, TNF, IFNA1, IFNB1, TNFSF14, PENK, ERVK-20, IL6, ERVW-1, CEACAM5, PML, CSF2, VEGFA, IFI16, IL4, ERVK-32, MUL1, PRKN, TLR9, IRF3, CBLL2, TG, NGF, BCL2, MDK, NXF1, EGR1, SEC14L2, FLNB, ACTB, TERT, EGFR, IL10, USO1, TLR2, KLK3, COL18A1, UBE2B, CASP3, IL13, HCFC1, FLT3LG, ITIH4, SLPI, AKT1, CASP8, CTCF, STAT3, ATRX, DUT, TH, STAT1, APP, HSPA8, HSPA4, CTNNB1, ESR1, PTGS2, FXN, LOC110013312, MAP2K7, GJA1, SST, TRAF3, RPL41, CRP, SLC5A5, CXCL8, CDK1, PPP1R15A, UNG, LTA, CD40, MAPK14, CAT, CGAS, TBC1D9, LGALS4, GEMIN4, CYTIP, MYBL2, HLA-DRB1, HLA-C, HLA-A, LAG3, ITGAL, DDX58, HBB, GZMB, KDR, MX1, IRF7, POLD1, HDAC5, ITGB2, NR3C1, ITPR1, TLR7, CFDP1, NFKB1, NHS, IL18, HDAC4, POLDIP2, IGHG3, DCAF1, IL11, GFAP, NFE2L2, MBL2, GRAP2, IL17A, HSP90AA1, IDO1, SH3KBP1, RNF19A, ABCB1, TBK1, INSM1, TREH, CD274, AHSA1, SENP1, AGFG1, HPRT1, SERPINA1, PILRA, FGF2, RIPK1, CDK9, CISH, SLC3A2, SLC2A1, VCP, CCL2, CRK, CSF1, TRPV1, GAD1, CX3CR1, CYP2B6, CYP4B1, DCK, RPAIN, CTTNBP2, BTLA, CD44, UNC93B1, CD40LG, ALB, TAP1, ARRB2, CCR2, ATM, MIR155, MIR145, BMP2, TLR4, SPARC, SP1, TRE-TTC3-1, IFNL1, CD80, CD34, DTYMK, EIF4H, SOCS1, BECN1, EPO, PRKRA, ROBO3, MTOR, PLAAT4, TNFSF11, F3, EIF4G2, EIF2AK2, NANOG, PSMD2, AIMP2, MAPK1, IL21, KDM4A, ABCC5, TOP2A, TRAF6, TNKS, NPEPPS, TMPO, CES2, KIF23, PROM1, SCLC1, HDAC9, TIMP2, THBD, AKT3, TIA1, HNRNPDL, TNFSF13, TNFSF15, TIMP3, SUCLA2, HS3ST1, TK2, MARCO, TRIM14, EIF2AK3, TNFRSF6B, BCLAF1, TYMS, AIM2, HIRA, CH25H, MTMR4, SLC6A5, USP7, ZAP70, MLRL, EEA1, XRCC5, NOLC1, MSC, PDLIM7, XPA, SMARCA5, PARG, VWF, SOCS3, IKBKG, VIM, HSPB3, KDM6A, MTMR3, TMPRSS11D, TYRO3, TYR, PSMG1, ARHGEF7, PAX8, MED23, FCGBP, SMC4, AAVS1, ABCB6, MED25, TRIM69, UPRT, RAET1E, HSPB6, PDZD8, ANTXR2, RAB39B, GPR146, TRS-TGA2-1, TRIM41, ZCCHC3, HAVCR2, PUS3, TRIM56, SENP7, TMX1, HM13, KCNIP4, TET1, AGBL2, SUGCT, GDPD3, HS3ST6, DCLRE1C, PJA1, XYLT2, LSM2, LRRC7, TICAM1, PYHIN1, GPBAR1, DDX53, MTCO2P12, ERVK-19, MYMX, IFNL4, RNA5SP141, ERVK-11, ERVK-18, ERVK-9, COMMD3-BMI1, KLRC4-KLRK1, POTEF, MIR21, MIR146A, MIR132, LINC01194, VHLL, NUPR2, STING1, BPIFA4P, STON1-GTF2A1L, CLEC9A, NEAT1, H19, IL27, TRIML2, NLRC3, RHOV, KIAA1210, PSMG2, TSPAN1, CD160, PHGDH, TOR1AIP1, SAMHD1, POU2F3, TRIM29, RCOR1, SMC5, KDM1A, RAB3GAP1, ATF6, KLRK1, MON1B, CHP1, ADRM1, IL36G, STON1, GTF2A1L, SPIN1, GADD45G, NES, POLQ, TNFSF13B, MCRS1, RACK1, NET1, ABCC4, CD96, G3BP1, PABPC1, RPUSD2, INTU, IGKV2D-10, ERBIN, ZNF415, NBPF1, LGR4, PRPF38B, AHI1, CPVL, IL17D, CHMP3, CXXC5, NCKIPSD, SLC25A37, SLC15A3, NT5C3A, HSPA14, LEF1, AADAT, DBR1, IRAK4, SIDT2, ASCC1, TRAT1, IL22, NOP53, PSAT1, PHPT1, HIPK2, ANKRD1, PTGER2, TGFB1, EIF2S1, GAD2, GABPA, XRCC6, FUT6, FUT3, FUS, FOS, FLT3, FGF1, FDXR, FCGR3B, FCGR3A, FASN, FANCD2, EZH2, ETV5, ETFA, ERCC6, EPHB4, EPHA3, EP300, SLC29A1, ENPEP, EMD, ELAVL3, EIF4G1, EIF4EBP1, EIF4E, EIF4A2, GH1, GJB1, CXCR3, HNRNPC, CCN1, IGF2, IGF1, IFNGR1, ICAM1, DNAJB1, HSPD1, HSPB2, HSPB1, HSPA9, HES1, HRG, TLX2, HMOX1, GRIN1, HMGA1, HMGB2, HMGB1, HLA-G, HLA-DQB1, HBZ, H2AX, GZMA, GUSB, GTF2H1, GRP, GRIN2D, GRIN2A, EPHA2, EGF, TRBV20OR9-2, EDN1, CCK, CASP9, CASP1, CAMP, CALR, CALCR, C3, BTK, BRCA2, BPHL, BMI1, BGLAP, BDNF, ADGRB1, ATR, ATF3, ASS1, ASNS, ASAH1, AR, FAS, APC, ANPEP, AKR1B1, AFM, ADSS2, GRK2, ADCYAP1R1, ACY1, CD19, CD28, CD86, CSH1, TOR1A, DUSP2, ATN1, DPP6, TIMM8A, DEFA5, DDX3X, DAXX, CYP2D6, CYP1A1, CTSB, CTLA4, CSH2, CRH, CD38, CPS1, COX8A, KLF6, COMT, CCR5, CCR1, ERCC8, CDX2, CDKN2A, CDKN1A, CDC34, CD68, CD47, IL1B, IL3, IL15, CXCL10, RPL22, RPL21, RPL11, RNASE1, REST, RBL2, RBBP6, RAG1, RAD51, PVR, PTPRC, PTGER4, PSMD13, PSMB8, PSEN1, PRTN3, PROS1, PRKD1, PRKCE, PPIB, CTSA, POU2F1, POMC, POLH, PLAU, PLAG1, PIK3CG, PIK3CD, PIK3CB, RPL26, RPL29, RPS11, SOAT1, TCF4, TBCE, TAF2, SUPT5H, SULT2A1, STAT6, STAT4, SRPK1, SPRR2A, SPR, SOX3, SOD2, SOD1, SNCA, RPS19, SMPD1, SLC22A1, SLC18A2, SLC6A8, SLC6A2, SFTPC, SELPLG, CXCL11, CCL5, CCL3, SCT, SALL1, RPS23, PIK3CA, SERPINF1, PECAM1, LMNA, MIP, CXCL9, MICE, MICB, MDM2, MAPT, MAL, SMAD4, SMAD3, EPCAM, LTF, LTBR, LMNB1, LIF, NR3C2, LHCGR, LGALS9, LGALS1, LBR, KNG1, KIR2DL2, JAK2, STT3A, ITGAV, ITGAM, IRS1, IRF2, INS, AFDN, MME, PDYN, NFKBIA, ENPP1, PDCD1, PCNA, PAX6, PAEP, CLDN11, ODC1, NUMA1, NTSR1, NTS, PNP, NOS2, NFYA, NFIX, MMP9, NFIC, NFIB, NFIA, NEDD4, NCL, MUC4, MUC1, COX2, MSI1, MSH2, MS, MRC1, MOG, H3P40

-
Chytridiomycosis
Wikipedia
B. dendrobatidis has been detected in 56 of 82 countries, and in 516 of 1240 (42%) species using a data set of more than 36,000 individuals. ... "Physiology of Batrachochytrium dendrobatidis , a chytrid pathogen of amphibians". Mycologia . 96 (1): 9–15. doi : 10.2307/3761981 . ... "Ecology: The proximate cause of frog declines?". Nature . 447 (7144): E4–E5. Bibcode : 2007Natur.447....4R . doi : 10.1038/nature05941 . ... Applied and Environmental Microbiology . 80 (13): 4034–4041. doi : 10.1128/AEM.04171-13 . ... "Treatment of chytridiomycosis with reduced-dose itraconazole" . Diseases of Aquatic Organisms . 99 (3): 243–249. doi : 10.3354/dao02475 .

-
Obesity Hypoventilation Syndrome
Wikipedia
CPAP alone is effective in more than 50% of people with OHS. [5] In some occasions, the oxygen levels are persistently too low ( oxygen saturations below 90%). In that case, the hypoventilation itself may be improved by switching from CPAP treatment to an alternate device that delivers "bi-level" positive pressure: higher pressure during inspiration (breathing in) and a lower pressure during expiration (breathing out). ... American Journal of Respiratory and Critical Care Medicine . 200 (3): e6–e24. doi : 10.1164/rccm.201905-1071ST . ... Breathing Disorders in Sleep . Saunders Ltd. pp. 80 . ISBN 978-0-7020-2510-5 . ^ Braunwald E (2005). ... The Report of an American Academy of Sleep Medicine Task Force" . Sleep . 22 (5): 667–89. doi : 10.1093/sleep/22.5.667 . PMID 10450601 . ^ Mokhlesi B, Kryger MH, Grunstein RR (February 2008). ... American Journal of Respiratory and Critical Care Medicine . 200 (3): e6–e24. doi : 10.1164/rccm.201905-1071ST .

-
Arsenic Poisoning
Wikipedia
] but reduction from +5 As to +3 As may be considered as a bioactivation [ clarification needed ] instead. [96] Another suggestion is that methylation might be a detoxification if "As[III] intermediates are not permitted to accumulate" because the pentavalent organoarsenics have a lower affinity to thiol groups than inorganic pentavalent arsenics. [95] Gebel (2002) stated that methylation is a detoxification through accelerated excretion. [97] With regard to carcinogenicity it has been suggested that methylation should be regarded as a toxification. [34] [98] [99] Arsenic, especially +3 As, binds to single, but with higher affinity to vicinal sulfhydryl groups , thus reacts with a variety of proteins and inhibits their activity. ... S2CID 24138885 . ^ a b Hughes, MF; Beck, BD; Chen, Y; Lewis, AS; Thomas, DJ (October 2011). ... "Cancer risks from arsenic in drinking water" . Environ. Health Perspect . 97 : 259–67. doi : 10.2307/3431362 . ... Atherosclerosis . 141 (2): 249–57. doi : 10.1016/S0021-9150(98)00178-6 . PMID 9862173 . ^ Dart, RC (2004). ... Toxicology and Applied Pharmacology . 183 (2): 99–107. doi : 10.1016/S0041-008X(02)99468-8 .CCL20, AQP9, SKIL, SOD2, SRP68, SSBP1, TRAPPC10, TNF, TNFAIP6, TP53, UBE2E1, PIAS1, USO1, IER3, USP13, CCRL2, CD83, MINPP1, AKAP9, ZNF267, N4BP2L2, RUFY3, TNIK, TRA2A, SOX18, ZFAND6, ZNF331, PELI1, AS3MT, TAF1D, MIR145, SFPQ, CCL3L3, CCL4, ATXN7, CD44, CRP, ERCC1, ERCC3, ERCC4, GOLGA4, CXCL2, CXCL3, HSPA1B, ID2, IL1A, IL1B, IL1RN, INPP5A, KCNJ2, KRT10, MT1A, MTHFR, GADD45B, NDUFB8, PNP, NR4A2, PDE4B, PFKFB3, PTX3, RFX3, RGS1, GSR, ALAD
-
Dihydrolipoamide Dehydrogenase Deficiency
Gene_reviews
Diagnosis Dihydrolipoamide dehydrogenase (DLD) functions as the E3 subunit of three mitochondrial enzyme complexes: branched-chain alpha-ketoacid dehydrogenase (BCKDH) complex, α-ketoglutarate dehydrogenase (αKGDH) complex, and pyruvate dehydrogenase (PDH) complex [Chuang et al 2013]. The E3 subunit is responsible for the reoxidation of the reduced lipoyl moiety of the E2 subunit. ... Molecular Genetic Testing Used in Dihydrolipoamide Dehydrogenase Deficiency View in own window Gene 1 Method Proportion of Pathogenic Variants 2 Detectable by Method DLD Sequence analysis 3 42/43 (98%) 4 Gene-targeted deletion/duplication analysis 5 Unknown 6 Targeted analysis for pathogenic variants 7 See footnote 8. 1. ... Nomenclature DLD deficiency is occasionally referred to as maple syrup urine disease (MSUD) type 3 as it functions as the E3 subunit of BCKDH. Note that MSUD type 1 is caused by biallelic pathogenic variants in BCKDHA (E1α) or BCKDHB (E1β) and MSUD type 2 is caused by biallelic pathogenic variants in DBT (E2). ... Prevalence In the Ashkenazi Jewish population, the carrier frequency of the c.685G>T (p.Gly229Cys) pathogenic variant is estimated to be between 1:94 and 1:110 with an estimated disease frequency of 1:35,000 to 1:48,000 [Scott et al 2010].
-
Traumatic Brain Injury
Wikipedia
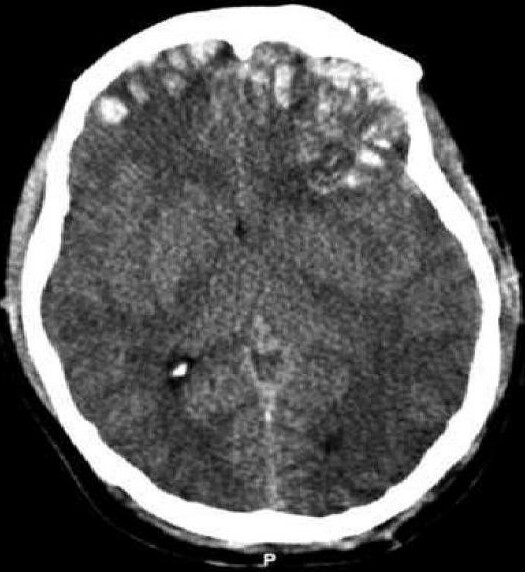
The most sensitive physical measure to date is the quantitative EEG, which has documented an 80% to 100% ability in discriminating between normal and traumatic brain-injured subjects. [82] [83] Neuropsychological assessment can be performed to evaluate the long-term cognitive sequelae and to aid in the planning of the rehabilitation . [75] Instruments range from short measures of general mental functioning to complete batteries formed of different domain-specific tests . ... An increase in use of helmets could reduce the incidence of TBI. [62] Due to the possibility that repeatedly "heading" a ball practicing soccer could cause cumulative brain injury, the idea of introducing protective headgear for players has been proposed. [85] Improved equipment design can enhance safety; softer baseballs reduce head injury risk. [86] Rules against dangerous types of contact, such as "spear tackling" in American football , when one player tackles another head first, may also reduce head injury rates. [86] Falls can be avoided by installing grab bars in bathrooms and handrails on stairways; removing tripping hazards such as throw rugs; or installing window guards and safety gates at the top and bottom of stairs around young children. [55] Playgrounds with shock-absorbing surfaces such as mulch or sand also prevent head injuries. [55] Child abuse prevention is another tactic; programs exist to prevent shaken baby syndrome by educating about the dangers of shaking children. [58] Gun safety, including keeping guns unloaded and locked, is another preventative measure. [87] Studies on the effect of laws that aim to control access to guns in the United States have been insufficient to determine their effectiveness preventing number of deaths or injuries. [88] Recent clinical and laboratory research by neurosurgeon Julian Bailes, M.D., and his colleagues from West Virginia University, has resulted in papers showing that dietary supplementation with omega-3 DHA offers protection against the biochemical brain damage that occurs after a traumatic injury. [89] Rats given DHA prior to induced brain injuries suffered smaller increases in two key markers for brain damage (APP and caspase-3), as compared with rats given no DHA. [90] “The potential for DHA to provide prophylactic benefit to the brain against traumatic injury appears promising and requires further investigation. ... This is done because the initial damage caused by trauma cannot be reversed. [94] Rehabilitation is the main treatment for the subacute and chronic stages of recovery. [94] International clinical guidelines have been proposed with the aim of guiding decisions in TBI treatment, as defined by an authoritative examination of current evidence . [9] Acute stage Tranexamic acid within three hours of a head injury decreases the risk of death. [95] Certain facilities are equipped to handle TBI better than others; initial measures include transporting patients to an appropriate treatment center. [51] [96] Both during transport and in hospital the primary concerns are ensuring proper oxygen supply, maintaining adequate blood flow to the brain, and controlling raised intracranial pressure (ICP), [10] since high ICP deprives the brain of badly needed blood flow [97] and can cause deadly brain herniation . ... Once medically stable, people may be transferred to a subacute rehabilitation unit of the medical center or to an independent rehabilitation hospital . [94] Rehabilitation aims to improve independent functioning at home and in society, and to help adapt to disabilities. [94] Rehabilitation has demonstrated its general effectiveness when conducted by a team of health professionals who specialize in head trauma. [123] As for any person with neurologic deficits, a multidisciplinary approach is key to optimizing outcome. ... Almost all people with mild TBI are able to live independently and return to the jobs they had before the injury, although a small portion have mild cognitive and social impairments. [87] Over 90% of people with moderate TBI are able to live independently, although some require assistance in areas such as physical abilities, employment, and financial managing. [87] Most people with severe closed head injury either die or recover enough to live independently; middle ground is less common. [9] Coma, as it is closely related to severity, is a strong predictor of poor outcome. [10] Prognosis differs depending on the severity and location of the lesion, and access to immediate, specialised acute management.
-
Influenza
Wikipedia
These different types of HA and NA form the basis of the H and N distinctions in, for example, H5N1 . [79] There are 18 H and 11 N subtypes known, but only H 1, 2 and 3, and N 1 and 2 are commonly found in humans. [80] [81] Replication Host cell invasion and replication by the influenza virus. ... Hence, the majority of newly manufactured influenza viruses are mutants; this causes antigenic drift , which is a slow change in the antigens on the viral surface over time. [91] The separation of the genome into eight separate segments of vRNA allows mixing or reassortment of vRNAs if more than one type of influenza virus infects a single cell. ... Also, when two or more viruses infect a cell, genetic variation may be generated by homologous recombination . [92] [93] Homologous recombination can arise during viral genome replication by the RNA polymerase switching from one template to another, a process known as copy choice. [93] Mechanism Transmission When an infected person sneezes or coughs more than half a million virus particles can be spread to those close by. [94] In otherwise healthy adults, influenza virus shedding (the time during which a person might be infectious to another person) increases sharply one-half to one day after infection, peaks on day 2 and persists for an average total duration of 5 days—but can persist as long as 9 days. [23] In those who develop symptoms from experimental infection (only 67% of healthy experimentally infected individuals), symptoms and viral shedding show a similar pattern, but with viral shedding preceding illness by one day. [23] Children are much more infectious than adults and shed virus from just before they develop symptoms until two weeks after infection. [95] In immunocompromised people, viral shedding can continue for longer than two weeks. [96] Influenza can be spread in three main ways: [97] [98] by direct transmission (when an infected person sneezes mucus directly into the eyes, nose or mouth of another person); the airborne route (when someone inhales the aerosols produced by an infected person coughing, sneezing or spitting) and through hand-to-eye, hand-to-nose, or hand-to-mouth transmission, either from contaminated surfaces or from direct personal contact such as a handshake. The relative importance of these three modes of transmission is unclear, and they may all contribute to the spread of the virus. [9] In the airborne route, the droplets that are small enough for people to inhale are 0.5 to 5 μm in diameter and inhaling just one droplet might be enough to cause an infection. [97] Although a single sneeze releases up to 40,000 droplets, [99] most of these droplets are quite large and will quickly settle out of the air. [97] How long influenza survives in airborne droplets seems to be influenced by the levels of humidity and UV radiation , with low humidity and a lack of sunlight in winter aiding its survival; [97] ideal conditions can allow it to live for an hour in the atmosphere. [100] As the influenza virus can persist outside of the body, it can also be transmitted by contaminated surfaces such as banknotes , [101] doorknobs, light switches and other household items. [27] The length of time the virus will persist on a surface varies, with the virus surviving for one to two days on hard, non-porous surfaces such as plastic or metal, for about fifteen minutes on dry paper tissues, and only five minutes on skin. [102] However, if the virus is present in mucus, this can protect it for longer periods (up to 17 days on banknotes). [97] [101] Avian influenza viruses can survive indefinitely when frozen. [103] They are inactivated by heating to 56 °C (133 °F) for a minimum of 60 minutes, as well as by acids (at pH <2). [103] Pathophysiology The different sites of infection (shown in red) of seasonal H1N1 versus avian H5N1 . ... Deaths worldwide Case fatality rate Pandemic severity 1889–90 flu pandemic [227] 1889–90 1.53 billion Likely H3N8 or H2N2 2.10 ( IQR , 1.9–2.4) [227] 20–60% [227] (300–900 million) 1 million 0.10–0.28% [227] 2 1918 flu [228] 1918–20 1.80 billion H1N1 1.80 (IQR, 1.47–2.27) 33% (500 million) [229] or >56% (>1 billion) [230] 17 [231] –100 [232] [233] million 2–3%, [230] or ~4%, or ~10% [234] 5 Asian flu 1957–58 2.90 billion H2N2 1.65 (IQR, 1.53–1.70) >17% (>500 million) [230] 1–4 million [230]DDX58, IFITM3, MX1, CXCL10, IRF7, LAMP3, CCL2, EIF2AK2, RSAD2, STAT1, ISG15, TNFSF10, IFIH1, PLSCR1, OAS2, IFIT5, ATF3, OAS1, IFI44L, TNFAIP6, APOL6, OASL, OAS3, DDX60, RTP4, HERC6, SLC22A8, IFI44, UBE2L6, ZCCHC2, SAMD9, XAF1, SERPING1, CCL8, SCO2, MX2, GBP1, PARP12, IFI6, HERC5, IFI27, IFIT3, XIST, TOR1B, IFI35, TRIM22, IFIT2, SIGLEC1, TDRD7, TREX1, IFIT1, LY6E, SFTPD, RAB39B, IL1B, IL2, IVNS1ABP, SARS2, ERVK-6, TNF, IFNG, IFNB1, IFNA13, IFNA1, PTPN11, IL10, ROBO3, PLAAT4, IL17A, SARS1, TLR4, IL6, HLA-A, PBRM1, TLR7, LINC01672, ERVK-32, TLR2, COPD, KRT31, CRP, ZMYND10, CD248, CPVL, TLR9, TLR3, VHLL, IRF3, HMOX1, CD40LG, MAPK1, LSAMP, IGHA1, IL22, ARIH1, CSF2, MAPK14, IL4, NLRP3, ACTB, PIK3CA, NR1I2, TRIM25, MED1, IL2RA, DOCK3, PPBP, ISG20, TMPRSS2, CASP1, ST14, IL33, GRN, PKD1, PEBP1, HLA-C, RNPC3, MYD88, NCR1, MAVS, DHX9, PRNP, MRC1, ACE2, GZMB, FOLH1, TRBV20OR9-2, MBL2, ICAM1, HSPA4, HCL2, RPS19, PIK3CG, IL27, POLDIP2, CCR5, CD28, GRAP2, CD80, CFTR, RNF19A, IL5, CRK, AHSA1, LOH19CR1, SRL, IL1A, CCR2, CXCL8, SARDH, PER2, AIMP2, IFNL1, ATN1, PIK3CD, IFNAR1, PIK3CB, EIF4G1, HLA-B, TLR5, PRDX2, CFH, HLA-DRB1, HMGB1, TNFRSF9, TXN, MYO1G, IL7R, ERVW-1, IL15, KRT32, NM, HCRT, EPHA3, NHS, EGFR, DHFR, ST6GAL1, CTLA4, RAB11A, CCL5, CD86, PLG, ANP32B, POTEF, CASP3, B3GAT1, CAP1, IL17D, C4BPA, PPARG, BST2, IRF9, ABCB6, ALB, CD274, PTGS2, SDS, CARD14, EPHB2, FPR2, MPO, SPINT1, CBLIF, CFAP97, GPI, SOD1, GABPA, XPO1, NFE2L2, COX2, MFAP1, FOXP3, IPO5, RELA, NS2, CMPK1, ICOS, PPIA, MMP9, SEC14L2, MPPE1, BRD4, LNPEP, LRIT1, TGFB1, NOS2, VTRNA1-1, STAT3, PAM, SEA, XCL1, GOLPH3, SERPINB6, LAMP1, LAMC2, MUC5AC, MUC1, SMS, MYDGF, NT5C2, PAGR1, RBM45, ANP32A, PRDM1, STING1, NR4A3, BCL2, AREG, EIF4A2, APRT, ESCO2, F2RL1, FGF2, MLANA, FN1, GAST, VTN, GALNS, GAPDH, RTL1, SLC9A6, CTAA1, TNFSF9, CD79A, HACD1, CDC42, IL18R1, SORBS1, TNFRSF18, MIR223, MBTPS1, NCR2, TNFSF13B, CLK1, IL32, CPT2, CD163, MIR155, MIR146A, RIPK3, ERVK-20, ABHD2, HLA-DQB1, TRAF6, DOT1L, TRAF3, MTCO2P12, ADAR, IFNA2, IFNAR2, IGF1, LINC02605, IL7, CXCR2, IL18, ILF3, ABO, ITGAE, ITGAM, SHCBP1, EBI3, TTR, TIRAP, LOC102724971, APCS, XCR1, BATF2, LOC102723407, ANXA1, UCK2, IL17F, SOCS3, MTSS2, ATG7, ZMPSTE24, RIDA, PRPF8, B3GNT3, FLVCR1, ATP2C1, RTN3, BET1, TRIM3, PPIE, DLL1, RBMS3, IL17C, CLEC10A, DISC1, TBK1, SLC35A1, IL37, NXF1, CFDP1, BAMBI, KHDRBS1, SLC27A4, IL24, TPPP, ADAMTS7, IRAK3, PADI4, CHP1, USP18, ARHGAP45, SRRM2, MORC3, ECD, P2RX2, SNRNP200, WDTC1, TRAM1, MPRIP, SIRT1, CLEC5A, BACE1, CXCR6, SLC27A5, PTPN22, CTCF, POLD3, PLK4, BACE2, CCL27, KLK5, LILRB1, MALT1, MCF2L, CPSF4, JTB, SUGT1, IL17RA, TMED2, CKAP4, SGK3, ABCA1, IL22RA1, CD207, MIR192, TICAM2, CCL4L1, PRSS57, LINC01194, MIR144, MIR15A, MIR184, MIR198, CYCSP51, MIR200C, MIR205, MIR206, MIR21, MIR29A, MIR29B1, MIR29B2, HLA-P, RAB7B, MIR30C1, NRSN1, TARS3, B4GALNT2, NMS, IL31RA, EGFLAM, ASZ1, TRIM69, MUC15, TREML4, TICAM1, DEFT1P, BCL6B, PTF1A, IFNL3, CLEC9A, BTBD8, MIR29C, MIR30C2, CTHRC1, ERVK-21, MFT2, MIR1260A, TMED7-TICAM2, PSMB8-AS1, P2RX5-TAX1BP3, ERVK-10, ERVK-9, ERVK-18, MIR744, ERVK-25, ERVK-24, MYMX, GATD3B, ERVK-19, CST12P, H3P24, EGOT, GGTLC4P, MIR31, MIR146B, MIR34A, MIR34C, DEFB103A, MIR328, ERVK-7, MIR451A, MIR485, MIR505, GGT2, ERVK-8, MIR483, GGTLC5P, H3P38, MIR449B, MUC5B, GGTLC3, IL22RA2, SLC46A1, GEMIN4, SMU1, UGT1A4, UGT1A1, UGT1A3, OTUD4, CASZ1, MARCHF1, NUDT11, PACC1, UGT1A5, ENAH, DEFB103B, LANCL2, CCL28, SPHK2, PNO1, SH3GLB2, UGT1A9, UGT1A6, CD177, BPIFA1, MBL3P, TMED5, TMED7, DYNC1LI1, LINC00328, VPS28, HSPA14, TLR8, UGT1A7, CRLF3, DDX41, ISYNA1, IL23A, DDIT4, UGT1A10, UGT1A8, CHPT1, AICDA, SCGB3A1, NLRC5, NDFIP1, NPL, ZBP1, UNC93B1, TLR10, TRIM56, PARP9, CHD6, DHDDS, GINS4, HOPX, MAK16, WNT3A, FRMD7, MCU, TRIM41, TARS2, NLRX1, GATAD2B, KLRG1, SEMA6A, ARHGAP21, SUGP1, HAMP, C6orf47, NLRC4, PRM3, HEATR6, DHX58, DMRTA1, TNMD, NOD2, CLEC7A, GORASP1, WNK1, WNK4, CALCOCO2, TARS1, DHRS2, ALYREF, GPT, CXCL1, CXCL2, GRP, PDIA3, GRSF1, GZMA, H1-2, HLA-DPB1, HMGCR, NR4A1, HNRNPK, HP, HPD, PRMT1, HES1, HSPA8, GPS1, CXCR3, GLRX, FUT2, EIF4E, EIF4G2, ENO1, ESR1, F2R, FCN2, FLT3LG, FYB1, GLDC, GAD1, GATA2, GATA3, GGT1, GH1, GLA, GLB1, HSPD1, TNC, IFNA6, EPCAM, KRT10, LAG3, LGALS9, LIF, LPO, BCAM, SH2D1A, SMAD3, KPNA4, MATN1, MAX, MBD1, MBP, MEFV, MAP3K5, MIF, KRT5, KPNA3, IFNGR1, ITGB2, IGHM, IL3, IL4R, CXCR1, IL13, INSR, IRF4, ITGB7, KPNA1, JAK3, KEL, KIR2DL1, KLK1, KLRB1, KLRC2, KLRD1, EIF4A1, S1PR1, DPEP1, CASP10, C3, C5, C5AR1, C6, CALCR, CAMK2B, CASP8, CAV1, BDNF, RUNX1T1, SERPINH1, CCK, CCND3, CCNT1, CD1A, CD2, CXCR5, BCR, CD14, ALK, ABL1, ACP3, AGA, JAG1, AHR, AKT1, ALDH2, ANXA2, BCL6, ANXA6, ANXA13, APC, BIRC3, XIAP, ARSF, BAG1, CD9, CD19, DYNC1LI2, CD55, CR2, CREB1, CREM, CSF3, CSF3R, CTNNB1, CYLD, DAP, CCR7, DDOST, DDX3X, DDX5, DEFA1, DEFB1, DLAT, DNM1, KLF6, CLCN7, CD27, CDK9, TNFRSF8, CD38, CD44, CD48, CD69, CD81, CDK1, CDKN1B, AP2M1, CDR1, CDSN, CEL, CENPF, CES1, AKR1C4, CISH, CXCL9, MIP, MPL, UGT1A, TIMP1, TNNI3, TOP1, TP53, HSP90B2P, TNFRSF4, TYR, KDM6A, TERT, UVRAG, VASP, VCP, VEGFA, VIM, BEST1, WAS, THBS1, TMBIM6, DNALI1, SNAI1, SRSF2, SRSF3, SFTPB, SGTA, ST3GAL3, SLC5A5, SLC20A1, SON, TCF7, SPR, ST13, STAT2, SYT1, TAP1, ABCA3, HNF1A, ZBTB25, CXCR4, SELL, CCL4L2, NTN1, GSTO1, AIM2, EIF2AK3, GAL3ST1, TECR, GOSR1, IKBKE, MAPKAPK2, SOCS5, NUP93, SPOCK2, TRIM14, SETDB1, BCAP31, TRIM28, TMPRSS11D, AURKB, RAB7A, PRPF18, DDX39B, PABPN1, IV, GATD3A, USP11, EPX, IFITM1, TP63, MYOM2, SOCS1, IL1RL2, SPHK1, HSPB3, CLDN2, P2RX6, PCSK7, SRSF1, SDC1, MSR1, PDR, PRDX1, SERPINE1, PAK1, PAX5, PDE7A, PDGFRB, PDPK1, PECAM1, PA2G4, PF4, ABCB1, PHB, PITX1, PKM, PKP2, PLS1, FURIN, P2RY2, POLR2A, CNOT4, COX1, MMUT, PPP1R12A, NAGA, NEU1, NFKBIB, NFKBIL1, NPY, P2RY1, NT5E, OSM, P2RX1, P2RX3, P2RX4, P2RX5, P2RX7, POLD1, POLR2B, CCL11, RPE65, PTK2, RAB5A, RAG1, RARA, RARB, DPF2, RNASE1, S100A8, PTEN, S100A11, SAA3P, SAFB, SAG, SATB1, CCL3, CCL4, PTGS1, PTBP1, POU1F1, MAP2K6, PPARA, PRD, PRKAA1, PRKAA2, PRKAB1, PRKCD, MAPK8, MAP2K7, PTAFR, PROC, PRSS8, PRTN3, PSMB8, PSMD2, PSMD4, PSMD10, H3P19

-
Health Effects Of Tobacco
Wikipedia
Carbon monoxide in tobacco smoke exerts negative effects by reducing the blood's ability to carry oxygen. [80] Smoking also increases the chance of heart disease , stroke , atherosclerosis , and peripheral vascular disease . [81] [82] Several ingredients of tobacco lead to the narrowing of blood vessels, increasing the likelihood of a blockage, and thus a heart attack or stroke. ... Smoking also increases blood pressure and weakens blood vessels. [91] Renal [ edit ] In addition to increasing the risk of kidney cancer, smoking can also contribute to additional renal damage. ... In a prospective study of community-dwelling people 60–90 years of age, during 1993, of unimmunized people 23% of smokers had clinical influenza as compared with 6% of non-smokers. [97] Smoking may substantially contribute to the growth of influenza epidemics affecting the entire population. [94] However, the proportion of influenza cases in the general non-smoking population attributable to smokers has not yet been calculated. [ citation needed ] Mouth [ edit ] Dental radiograph showing bone loss in a 32 year old heavy smoker. ... The National Institutes of Health , through the National Cancer Institute , determined in 1998 that "cigar smoking causes a variety of cancers including cancers of the oral cavity (lip, tongue, mouth, throat), esophagus , larynx , and lung ." [90] Pipe smoking involves significant health risks, [98] [99] particularly oral cancer. [100] Roughly half of periodontitis or inflammation around the teeth cases are attributed to current or former smoking. Smokeless tobacco causes gingival recession and white mucosal lesions . Up to 90% of periodontitis patients who are not helped by common modes of treatment are smokers.

-
Lymphangioleiomyomatosis
Wikipedia
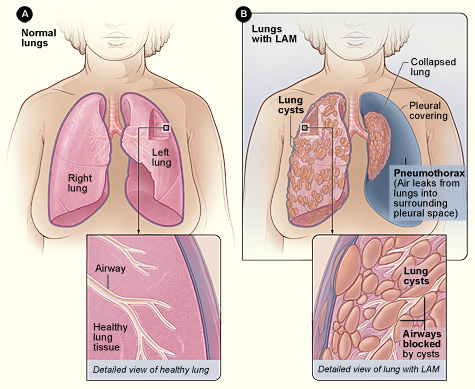
A review of the CT by an expert familiar with LAM may increase diagnostic accuracy. [80] Chylothorax can also bring LAM to attention. ... In patients with TSC, nodular densities on HRCT may represent multifocal micronodular pneumocyte hyperplasia (MMPH) made up of clusters of hyperplastic type II pneumocytes. [79] [88] [89] MMPH may be present in males or females with TSC in the presence or absence of LAM, but not in patients with S-LAM. [90] MMPH is not typically associated with physiologic or prognostic consequences, but one case of respiratory failure due to MMPH has been reported. [91] [92] [93] Ventilation-perfusion scans [ edit ] In one study ventilation-perfusion scans were abnormal in 34 of 35 LAM patients. [5] The most common abnormality was nonspecific diffuse heterogeneity , usually grossly matched. ... Approximately 25% of patients with obstructive physiology may demonstrate bronchodilator responsiveness but may be less in more severe obstruction. [99] [100] The obstructive physiologic defect in LAM is primarily attributable to airflow obstruction. [101] The earliest change in initial pulmonary function testing in various case series was abnormal gas transfer, as assessed by the diffusing capacity for carbon monoxide (DLCO), described in 82% to 97% of patients. [3] [4] [6] It is not unusual for DLCO to be reduced out of proportion to forced expiratory volume in 1 second (FEV1). [99] Reduction in DLCO and increase in residual volume are generally considered to be LAM's earliest physiologic manifestations. [ citation needed ] Cardiopulmonary exercise testing in a much larger cohort of patients with LAM revealed a reduced maximal oxygen consumption ( VO 2 max ) and anaerobic threshold in 217 patients. [102] [103] Exercise-induced hypoxemia was found even in patients who did not have resting abnormalities in FEV1 and DLCO. ... PMID 10499073 . ^ a b c Johnson, SR; Tattersfield, AE (2000). "Clinical experience of lymphangioleiomyomatosis in the UK" . ... Respir. Cell Mol. Biol . 34 (4): 473–80. doi : 10.1165/rcmb.2005-0374OC .TSC2, TSC1, VEGFD, HES1, JAG2, MTOR, SLC12A3, TESC, ACTB, RPS6KB1, ESR1, MMP2, REN, VEGFA, EGFR, EGF, SRF, ACE, PTGS2, IGFBP2, IGF1, PLAU, MAPK1, IGF2, CTNNB1, VEGFC, A1BG, TNF, TIMP3, YWHAZ, SPP1, SOX9, SMN2, SMN1, STAT3, HMGA2, AIMP2, CD274, SFTPA1, MIR21, COPD, PLB1, UBASH3B, COL18A1, PDGFC, ING4, POLDIP2, FOSL1, RNF19A, PLAAT3, PDPN, AHSA1, GPNMB, GGPS1, GRAP2, SFTPD, PMEL, PLG, SELL, CRK, EPHB2, EDN1, DES, CYP19A1, CTSK, CTLA4, MAPK14, CPT1A, CXCL5, CD44, DDR1, BSG, ANXA6, ALDH1A1, AGT, PARP1, GC, GJA1, IFNA1, IFNA13, CCL2, RPS6, PRL, PLA2G1B, PDCD1, SERPINE1, TNFRSF11B, DDR2, MMP14, MMP9, MMP7, MMP1, LMNA, LGALS3, IFNB1, SFTPA2
-
Wrist Osteoarthritis
Wikipedia
"Wrist osteoarthritis". Scand J Surg . 97 (4): 305–9. doi : 10.1177/145749690809700406 . ... The Journal of Hand Surgery . 15 (6): 847–854. doi : 10.1016/0363-5023(90)90002-9 . PMC 2328843 . PMID 2269772 . ^ Inglis, AE; Jones, EC (1977). ... The Journal of Hand Surgery . 15 (3): 426–430. doi : 10.1016/0363-5023(90)90054-U . PMID 2348060 . ^ Tomaino, MM; Delsignore, J; Burton, RI (1994). ... The Journal of Hand Surgery . 19A (4): 694–703. doi : 10.1016/0363-5023(94)90284-4 . PMID 7963335 . ^ DiDonna, ML; Kiefhaber, TR; Stern, PJ (2004). ... PMID 7722266 . ^ Anderson, MC; Adams, BD (2005). "Total wrist arthroplasty".

-
Rabies
Wikipedia
But rabies is common among wild animals in the United States, and an average of 100 dogs become infected from other wildlife each year. [90] [91] Bats , raccoons , skunks and foxes account for almost all reported cases (98% in 2009). ... An extensive wild animal vaccination campaign eliminated the virus from Italy again, and it regained the rabies-free country status in 2013, the last reported case of rabies being reported in a red fox in early 2011. [96] [97] The United Kingdom has been free of rabies since the early 20th century except for a rabies-like virus in a few Daubenton's bats . ... The last infection in the UK occurred in 1922, and the last death from indigenous rabies was in 1902. [98] [99] Unlike many of the other countries of Europe it is protected by being an island, and by strict quarantine procedures. ... The World of the Fox . Vancouver: Greystone Books. pp. 94–5 . ISBN 978-0-87156-377-4 . ^ "Rabies in the U.S." ... "Current and future approaches to the therapy of human rabies" . Antiviral Research (Review). 99 (1): 61–67. doi : 10.1016/j.antiviral.2013.01.003 .THBS1, IL6, IFNA1, PTPN22, TLR3, PREP, PAEP, IFNA13, ERVK-6, LAMP3, OCA2, LSAMP, EGFLAM, MALT1, MECP2, MAP2K7, ERVK-20, TNF, MYOM2, ERVW-1, ALB, HPSE, RECQL4, ENOSF1, EPHB6, DNLZ, RAB7A, UBE2B, RNGTT, AKT1, UBA7, ARHGEF7, TCEA1, STAT3, STAT1, SOAT1, CCL21, CCL5, SARS1, RAB5A, TNFSF13, TNFSF13B, CH25H, CBFA2T2, PERCC1, MTRNR2L10, MIR455, MIR423, RAB7B, CBLL2, DCD, RSAD2, MUL1, TNIP2, SAGE1, SARS2, PPP1R12C, TFPT, SGSM3, ERAL1, PIP5K1C, PPP1R13B, CXCL13, HDAC6, ISG15, MAPK3, PIK3CD, POU3F4, PIK3R2, IFNB1, IFIT2, ICAM1, HSPA8, AGFG1, HMGB1, GRM2, GFAP, GAS1, FUT2, FN1, ESR1, EPHA3, DUSP5, SLC26A3, CYP3A4, CYP2D6, CYP2C9, CYP1A2, CSF2, MAP3K8, CHRNA4, CASP2, VPS51, ANGPT2, IFNG, IGF1, IGHA1, MYC, PIK3R1, PIK3CG, PIK3CB, PIK3CA, PDR, PCBP2, PRKN, NTS, NGFR, NEFH, NEDD4, MTM1, IGHG3, MOG, MAP2, LAMP1, KPNA4, ITGB1, IRF3, CXCL10, IL7, IL5, IL1A, IGKV@, ERVK-32

-
Polycystic Ovary Syndrome
Wikipedia
A newer insulin resistance medication class, the thiazolidinediones (glitazones), have shown equivalent efficacy to metformin, but metformin has a more favorable side effect profile. [85] [86] The United Kingdom's National Institute for Health and Clinical Excellence recommended in 2004 that women with PCOS and a body mass index above 25 be given metformin when other therapy has failed to produce results. [87] [88] Metformin may not be effective in every type of PCOS, and therefore there is some disagreement about whether it should be used as a general first line therapy. [89] In addition to this, metformin is associated with several unpleasant side effects: including abdominal pain, metallic taste in the mouth, diarrhoea and vomiting. [90] The use of statins in the management of underlying metabolic syndrome remains unclear. [91] It can be difficult to become pregnant with PCOS because it causes irregular ovulation . ... PMID 28531286 . ^ a b Crosignani PG, Nicolosi AE (2001). "Polycystic ovarian disease: heritability and heterogeneity" . ... "Renaming PCOS—a two-state solution" . J. Clin. Endocrinol. Metab . 98 (11): 4325–8. doi : 10.1210/jc.2013-2040 . ... "A meta-analysis of polycystic ovary syndrome in women taking valproate for epilepsy". Epilepsy Res . 97 (1–2): 73–82. doi : 10.1016/j.eplepsyres.2011.07.006 . ... "The clinical evaluation of hirsutism". Dermatol Ther . 21 (5): 376–91. doi : 10.1111/j.1529-8019.2008.00219.x .
-
Nance–horan Syndrome
Wikipedia
Contents 1 Presentation 2 Genetics 3 Diagnosis 4 Management 5 History 6 References 7 External links Presentation [ edit ] Dental features: [ citation needed ] small teeth in males pointed (screwdriver shaped or conical) incisors (sometimes called Hutchinson teeth) incisors with an irregulal incisal edge canines : enlarged and globular; may be dome or bud shaped with trilobed edge premolars and molars : small, round and globular; may have supernumary lobes (mulberry or lotus flower shape) widely separated teeth ( diastemma ) hypoplastic enamel dental agenesis presence of mesiodents (median incisor behind normal upper incisors) pulp chamber anomalies Facial features: [ citation needed ] anteverted pinnae long face prominent nasal bridge and nose prognathism occasionally Ophthalmic features: [ citation needed ] bilateral congenital nuclear opacities (100%) severe amblyopia nystagmus (93%) strabismus (43%) microcornea (96%) congenital glaucoma scleral staphylomas retinal cystoid degeneration microphthalmia These lead to severe visual impairment in affected males. Other: The fourth metacarpal may be shortened 30% of patients also have some degree of intellectual impairment: of these 80% are mildly to moderately affected: the other 20% may have developmental delays and behavior problems. [ citation needed ] Carrier females display milder variable symptoms of disease. Ocular signs are present in 90% of heterozygous females. These are typically lens opacities often involving the posterior Y sutures. ... Journal of Paediatrics and Child Health . 10 (2): 98–102. doi : 10.1111/j.1440-1754.1974.tb01098.x . ^ Nance, WE; Warburg, M; Bixler, D; Helveston, EM (1974). ... Birth Defects Original Article Series . 10 (4): 285–91. PMID 4470901 . External links [ edit ] Classification D ICD - 10 : Q87.0 MeSH : C538336 C538336, C538336 External resources Orphanet : 627 v t e Diseases of the human eye Adnexa Eyelid Inflammation Stye Chalazion Blepharitis Entropion Ectropion Lagophthalmos Blepharochalasis Ptosis Blepharophimosis Xanthelasma Ankyloblepharon Eyelash Trichiasis Madarosis Lacrimal apparatus Dacryoadenitis Epiphora Dacryocystitis Xerophthalmia Orbit Exophthalmos Enophthalmos Orbital cellulitis Orbital lymphoma Periorbital cellulitis Conjunctiva Conjunctivitis allergic Pterygium Pseudopterygium Pinguecula Subconjunctival hemorrhage Globe Fibrous tunic Sclera Scleritis Episcleritis Cornea Keratitis herpetic acanthamoebic fungal Exposure Photokeratitis Corneal ulcer Thygeson's superficial punctate keratopathy Corneal dystrophy Fuchs' Meesmann Corneal ectasia Keratoconus Pellucid marginal degeneration Keratoglobus Terrien's marginal degeneration Post-LASIK ectasia Keratoconjunctivitis sicca Corneal opacity Corneal neovascularization Kayser–Fleischer ring Haab's striae Arcus senilis Band keratopathy Vascular tunic Iris Ciliary body Uveitis Intermediate uveitis Hyphema Rubeosis iridis Persistent pupillary membrane Iridodialysis Synechia Choroid Choroideremia Choroiditis Chorioretinitis Lens Cataract Congenital cataract Childhood cataract Aphakia Ectopia lentis Retina Retinitis Chorioretinitis Cytomegalovirus retinitis Retinal detachment Retinoschisis Ocular ischemic syndrome / Central retinal vein occlusion Central retinal artery occlusion Branch retinal artery occlusion Retinopathy diabetic hypertensive Purtscher's of prematurity Bietti's crystalline dystrophy Coats' disease Sickle cell Macular degeneration Retinitis pigmentosa Retinal haemorrhage Central serous retinopathy Macular edema Epiretinal membrane (Macular pucker) Vitelliform macular dystrophy Leber's congenital amaurosis Birdshot chorioretinopathy Other Glaucoma / Ocular hypertension / Primary juvenile glaucoma Floater Leber's hereditary optic neuropathy Red eye Globe rupture Keratomycosis Phthisis bulbi Persistent fetal vasculature / Persistent hyperplastic primary vitreous Persistent tunica vasculosa lentis Familial exudative vitreoretinopathy Pathways Optic nerve Optic disc Optic neuritis optic papillitis Papilledema Foster Kennedy syndrome Optic atrophy Optic disc drusen Optic neuropathy Ischemic anterior (AION) posterior (PION) Kjer's Leber's hereditary Toxic and nutritional Strabismus Extraocular muscles Binocular vision Accommodation Paralytic strabismus Ophthalmoparesis Chronic progressive external ophthalmoplegia Kearns–Sayre syndrome palsies Oculomotor (III) Fourth-nerve (IV) Sixth-nerve (VI) Other strabismus Esotropia / Exotropia Hypertropia Heterophoria Esophoria Exophoria Cyclotropia Brown's syndrome Duane syndrome Other binocular Conjugate gaze palsy Convergence insufficiency Internuclear ophthalmoplegia One and a half syndrome Refraction Refractive error Hyperopia Myopia Astigmatism Anisometropia / Aniseikonia Presbyopia Vision disorders Blindness Amblyopia Leber's congenital amaurosis Diplopia Scotoma Color blindness Achromatopsia Dichromacy Monochromacy Nyctalopia Oguchi disease Blindness / Vision loss / Visual impairment Anopsia Hemianopsia binasal bitemporal homonymous Quadrantanopia subjective Asthenopia Hemeralopia Photophobia Scintillating scotoma Pupil Anisocoria Argyll Robertson pupil Marcus Gunn pupil Adie syndrome Miosis Mydriasis Cycloplegia Parinaud's syndrome Other Nystagmus Childhood blindness Infections Trachoma Onchocerciasis v t e Optical illusions ( list ) Illusions Afterimage Ambiguous image Ames room Barberpole Bezold Café wall Checker shadow Chubb Cornsweet Delboeuf Ebbinghaus Ehrenstein Flash lag Fraser spiral Gravity hill Grid Hering Impossible trident Jastrow Lilac chaser Mach bands McCollough Müller-Lyer Necker cube Orbison Penrose stairs Penrose triangle Peripheral drift Poggendorff Ponzo Rubin vase Sander Schroeder stairs Shepard tables Spinning Dancer Ternus Vertical–horizontal White's Wundt Zöllner Popular culture Op art Trompe-l'œil Spectropia (1864 book) Ascending and Descending (1960 drawing) Waterfall (1961 drawing) The dress (2015 photograph) Related Accidental viewpoint Auditory illusions Tactile illusions Temporal illusion
















