Loiasis is a form of filariasis (see this term), caused by the parasitic worm Loa loa , endemic to the forest and savannah regions of Central and Western Africa. Loiasis may either be asymptomatic or manifest as a large, transient area of localized, non-erythematous subcutaneous edema (Calabar swellings), adult worm migration through the sub-conjunctiva (''African eye worm'') and pruritus. Generalized itching, hives, muscle pains, arthralgias, fatigue, and adult worms visibly migrating under the surface of the skin may be observed. Severe complications such as encephalopathy have been reported in highly infected individuals receiving ivermectin during mass drug administration programs for the control of onchocerciasis and lymphatic filariasis (see these terms).
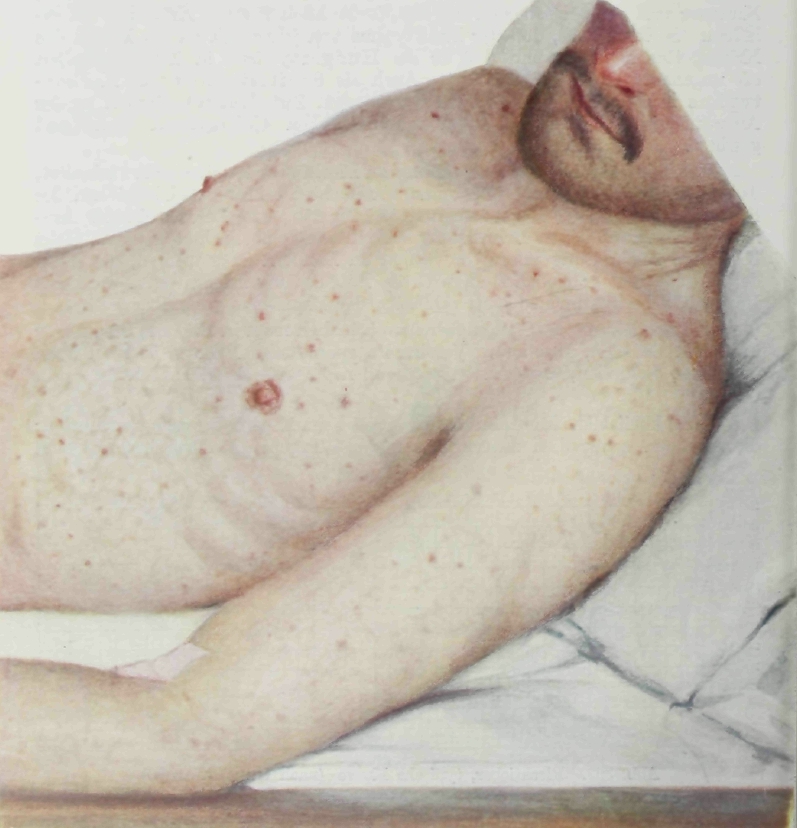
A Rickettsial disease characterized by malaise and vague symptoms before the onset of high fever, headache, severe myalgias and less commonly petechial rash on the trunk and limbs, nausea, vomiting, coughing and pneumonia. Most patients also have some central nervous system disturbances, such as meningeal irritation, confusion, drowsiness, seizures, coma, and hearing loss.
Nonetheless, it must be concluded that second-impact syndrome is an infrequent finding, predominately involving young athletes, and only rarely is fatal. [9] [10] [11] Dangers associated with repeated concussions [ edit ] Repeated concussions have been linked to a variety of neurological disorders among athletes, including chronic traumatic encephalopathy (CTE), Alzheimer's Disease , Parkinsonism and Amyotrophic lateral sclerosis (ALS). [12] [13] Repeated concussions or mild-to-moderate traumatic brain injuries (TBI) have also been established to have effects on the motor dysfunction and movement disorders, however a systematic review has concluded that more investigation is needed to fully understand the long term effects of concussions and TBIs. [14] Other risks [ edit ] In addition, returning to sports with impaired sensorimotor function after experiencing a sports-related concussion (SRC) increases the risk of sustaining musculoskeletal (MSK) injuries. [15] In addition, athletes that experienced a concussion are two times more likely to sustain an MSK injury compared to non-concussed athletes. [16] Incidence [ edit ] It is estimated that as many as 1.6–3.8 million concussions occur in the US per year in competitive sports and recreational activities; this is a rough estimate, since as many as 50% of concussions go unreported. [17] Concussions occur in all sports with the highest incidence in American football, ice hockey, rugby, soccer, and basketball. [4] In addition to concussions caused by a single severe impact, multiple minor impacts may also cause brain injury. [18] Less than 10% of cases experience a loss of consciousness, and many typical symptoms appear after the initial concussion evaluation. [19] The overall incidence risk of concussion is higher in adults than in youth, as the injury rate per 1,000 athletic exposures for youth is 0.23, compared to 0.28 in collegiate athletes. [20] Athlete-Based Concussion Rates Among National Collegiate Athletic Association Student-Athletes in Collegiate Sports [21] [ edit ] Sport Rates per 1000 Athlete-Exposures (95% Confidence Interval) Overall Competition Practice Men's Baseball 0.09 0.16 0.04 Basketball 0.38 0.53 0.34 Football 0.75 3.25 0.48 Ice hockey 0.74 2.40 0.20 Lacrosse 0.30 0.91 0.19 Soccer 0.26 0.67 0.14 Wrestling 0.89 4.31 0.48 Women's Basketball 0.53 1.00 0.39 Ice hockey 0.78 2.11 0.31 Lacrosse 0.45 1.28 0.25 Soccer 0.54 1.65 0.18 Softball 0.26 0.42 0.18 Volleyball 0.37 0.64 0.27 American Football [ edit ] Main article: Concussions in American football American football causes 250,000 concussions annually, and 20% of high-school football players experience a concussion every year. [22] [23] In 2000, researchers from the Sports Medicine Research Laboratory at the University of North Carolina at Chapel Hill analyzed 17,549 players from 242 different schools. 888 (5.1%) of the players analyzed have at least one concussion a season, and 131 (14.7%) of them have had another concussion the year later.
Frontotemporal dementia with parkinsonism-17 (FTDP-17) is a brain disorder. It is part of a group of conditions, called frontotemporal dementia or frontotemporal degeneration, that are characterized by a loss of nerve cells (neurons ) in areas of the brain called the frontal and temporal lobes. Over time, a loss of these cells can affect personality, behavior, language, and movement. The signs and symptoms of FTDP-17 usually become noticeable in a person's forties or fifties. Most affected people survive 5 to 10 years after the appearance of symptoms, although a few have survived for two decades or more.
Frontotemporal dementias (FTDs) are a group of neurodegenerative disorders associated with shrinking of the frontal and temporal anterior lobes of the brain. Symptoms include marked changes in social behavior and personality, and/or problems with language. People with behavior changes may have disinhibition (with socially inappropriate behavior), apathy and loss of empathy, hyperorality (eating excessive amounts of food or attempting to consume inedible things), agitation, compulsive behavior, and various other changes. Examples of problems with language include difficulty speaking or understanding speech. Some people with FTD also develop a motor syndrome such as parkinsonism or motor neuron disease (which may be associated with various additional symptoms).
Overview Frontotemporal dementia is an umbrella term for a group of brain disorders that primarily affect the frontal and temporal lobes of the brain. These areas of the brain are generally associated with personality, behavior and language. In frontotemporal dementia, portions of these lobes shrink (atrophy). Signs and symptoms vary, depending on which part of the brain is affected. Some people with frontotemporal dementia have dramatic changes in their personalities and become socially inappropriate, impulsive or emotionally indifferent, while others lose the ability to use language properly.
Frontotemporal dementia (FTD) comprises a group of neurodegenerative disorders, characterized by progressive changes in behavior, executive dysfunction and language impairment, as a result of degeneration of the medial prefrontal and frontoinsular cortices. Four clinical subtypes have been identified: semantic dementia, progressive non-fluent aphasia, behavioral variant FTD and right temporal lobar atrophy (see these terms).
Summary Clinical characteristics. The spectrum of GRN frontotemporal dementia ( GRN -FTD) includes the behavioral variant (bvFTD), primary progressive aphasia (PPA; further subcategorized as progressive non-fluent aphasia [PNFA] and semantic dementia [SD]), and movement disorders with extrapyramidal features such as parkinsonism and corticobasal syndrome (CBS). A broad range of clinical features both within and between families is observed. The age of onset ranges from 35 to 87 years. Behavioral disturbances are the most common early feature, followed by progressive aphasia. Impairment in executive function manifests as loss of judgment and insight. In early stages, PPA often manifests as deficits in naming, word finding, or word comprehension.
A number sign (#) is used with this entry because of evidence that frontotemporal dementia mapping to chromosome 3 is caused by heterozygous mutation in the CHMP2B gene (609512) on chromosome 3p11. Mutation in the CHMP2B gene can also cause a form of amyotrophic lateral sclerosis (ALS17; 614696). Description A substantial minority of degenerative dementias, perhaps 10%, lack the distinctive pathologic features that allow subclassification as Alzheimer disease (see 104300) or other forms of dementia. In perhaps half of these cases of nonspecific dementia, there is a positive family history of dementia, with an apparent autosomal dominant mode of inheritance. See also frontotemporal lobe dementia (FLDEM; 600274), which maps to chromosome 17 and is caused by mutation in the microtubule-associated protein tau gene (MAPT; 157140).