Load FindZebra Summary
Disclaimer:
FindZebra Search conducts a search using our specialized medical search engine.
FindZebra Summary uses the text completions API
(subject to OpenAI’s API data usage policies)
to summarize and reason about the search results.
The search is conducted in publicly available information on the Internet that we present “as is”.
You should be aware that FindZebra is not supplying any of the content in the search results.
FindZebra Summary is loading...
-
Trisomy 18
MedlinePlus
Causes Most cases of trisomy 18 result from having three copies of chromosome 18 in each cell in the body instead of the usual two copies. The extra genetic material disrupts the normal course of development, causing the characteristic features of trisomy 18. Approximately 5 percent of people with trisomy 18 have an extra copy of chromosome 18 in only some of the body's cells. ... Affected individuals have two copies of chromosome 18, plus the extra material from chromosome 18 attached to another chromosome. People with this genetic change are said to have partial trisomy 18. If only part of the q arm is present in three copies, the physical signs of partial trisomy 18 may be less severe than those typically seen in trisomy 18. ... Partial trisomy 18 can be inherited. An unaffected person can carry a rearrangement of genetic material between chromosome 18 and another chromosome.
-
Ring Chromosome 18
Wikipedia
Unsourced or poorly sourced material may be challenged and removed . Find sources: "Ring chromosome 18" – news · newspapers · books · scholar · JSTOR ( March 2017 ) Ring chromosome 18 Other names Ring chromosome 18 [1] Specialty Medical genetics Ring chromosome 18 is a genetic condition caused by a deletion of the two ends of chromosome 18 followed by the formation of a ring-shaped chromosome. ... This variation is also partly attributable to the incidence of mosaicism , which is relatively common in people with ring 18. Septal defect Holoprosencephaly has been reported in some people with ring 18. [5] This is due to the deletion of the TGIF gene on the short arm of chromosome 18 in some people with ring 18. [6] Approximately 30-40% of people with ring 18 have a congenital heart anomaly . ... Hypotonia is frequently seen in the ring 18 population. Seizures , though uncommon, have been reported in people with ring 18. ... Genetic [ edit ] Formation of a ring chromosome. Individuals with ring 18 have one of their two copies of chromosome 18 that has formed the shape of a ring. ... A ring-shaped chromosome is the result. In the case of ring 18, one of the two copies of chromosome 18 has formed a ring.
-
Trisomy 18
Orphanet
Trisomy 18 is a chromosomal abnormality associated with the presence of an extra chromosome 18 and characterized by growth delay, dolichocephaly, a characteristic facies, limb anomalies and visceral malformations. ... Etiology The majority of cases are associated with free trisomy 18. Mosaic trisomy 18 has been detected in a few patients presenting with a clinical picture that varies from classical trisomy 18 to a normal phenotype depending on the number of trisomic cells present in the tissues. The trisomy 18 phenotype appears to be associated with the presence of three copies of the 18q11-q12 interval. ... Genetic counseling The risk of recurrence of trisomy (21, 13 or 18) in families of an index case with trisomy 18 is around 1%. However, in families in which trisomy 18 is caused by translocation, the recurrence risk is higher if one of the parents is a carrier of a balanced translocation.AFP, PAPPA, BCL2, IGH, BCL6, MALT1, ADAM12, AFA, TTC3, PGF, SERPINB5, RPL17, TERC, TP53, VAPA, ZFY, PAEP, CKAP2, LGALS13, CHD7, CNDP2, RETN, CGB5, CGB8, SERPINB2, MYC, NOTCH1, DCC, ANPEP, BIRC3, APOA1, APOE, CD38, CDC25C, CGA, CGB3, FPR1, NEUROD2, FUT1, GH1, GHR, HTC2, IGHG3, KCNMA1, CD200, MTHFR, APCDD1
-
Ring Chromosome 18
GARD
Ring chromosome 18 is a rare chromosome abnormality in which the ends (arms) of chromosome 18 join together to form a ring shape. ... While most people with ring chromosome 18 have the ring chromosome in all of their body cells, some people also have some body cells with normal chromosomes (this is called mosaicism). People with ring chromosome 18 mosaicism may have milder symptoms. ... Ring chromosome 18 usually occurs sporadically (by chance) during the formation of egg or sperm cells or shortly after the egg and sperm join together. ... A chromosome test of the parents can help determine whether it was inherited and whether future children have an increased chance to have a chromosome abnormality. Treatment for ring chromosome 18 depends on the signs and symptoms present in each person.
-
Corticosterone Methyloxidase Type I Deficiency
OMIM
Description CMO type I deficiency is an autosomal recessive disorder caused by a defect in the penultimate biochemical step of aldosterone biosynthesis, the 18-hydroxylation of corticosterone (B) to 18-hydroxycorticosterone (18-OHB). ... In CMO I deficiency, aldosterone is undetectable, whereas its immediate precursor, 18-OHB, is low or normal. These patients have an increased ratio of corticosterone to 18-OHB (Portrat-Doyen et al., 1998). The CYP11B2 gene product also catalyzes the final step in aldosterone biosynthesis: the 18-oxidation of 18-OHB to aldosterone. ... In CMO II deficiency, aldosterone can be low or normal, but at the expense of increased secretion of 18-OHB. These patients have a low ratio of corticosterone to 18-OHB (Portrat-Doyen et al., 1998). ... The findings were consistent with a defect in 18-hydroxylation of corticosterone, thus confirming the diagnosis of CMO type I deficiency.
-
Corticosterone Methyloxidase Type Ii Deficiency
OMIM
Description CMO type II deficiency is an autosomal recessive disorder caused by a defect in the final biochemical step of aldosterone biosynthesis, the 18-hydroxylation of 18-hydroxycorticosterone (18-OHB) to aldosterone. ... These patients have a low ratio of corticosterone to 18-OHB (Portrat-Doyen et al., 1998). The CYP11B2 gene product also catalyzes an earlier step in aldosterone biosynthesis: the 18-hydroxylation of corticosterone to 18-OHB. ... The enzymatic defect was in the final conversion of 18-hydroxycorticosterone to aldosterone. ... The authors postulated a defect in 18-OH-dehydrogenase. Spontaneous improvement occurred.
-
Trisomy 18-Like Syndrome
OMIM
Clinical Features Shashi et al. (1996) described a newborn infant with first-cousin parents who had a complex congenital heart defect and minor anomalies suggestive of trisomy 18. Blood lymphocyte and skin fibroblast karyotypes were normal. ... On interphase fluorescence in situ hybridization (FISH) using autopsy specimens, a significant number of cells in the liver (17%) were trisomic for chromosome 18, compared to normal controlled liver tissue. ... Shashi et al. (1996) concluded that the apparent mosaicism for trisomy 18 in the liver may have been spurious, and that the pattern of anomalies, together with the parental consanguinity, may indicate a new autosomal recessive malformation syndrome. ... Eyes - Narrow palpebral fissures - Telecanthus Inheritance - Autosomal recessive Lab - ? mosaicism for trisomy 18 in the liver Mouth - Micrognathia Nose - Broad nasal root - Deficient alae nasi Cardiac - Complex congenital heart defect Ears - Low-set ears - Malformed ears - Preauricular tags ▲ Close
-
Chromosome 18 Pericentric Inversion
OMIM
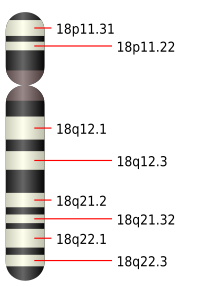
A number sign (#) is used with this entry because a chromosome 18 pericentric inversion can result in a recombinant dup(18p)/del(18q) or dup(18q)/del(18p) phenotype. Cytogenetics Mejia-Baltodano et al. (1997) reported a family in which the father had a large pericentric inversion of chromosome 18 (p11.2q22). The oldest daughter had a dup(18q)/del(18p) recombinant, whereas her younger sister and brother had a dup(18p)/del(18q) recombinant. ... Vermeulen et al. (2005) described a family segregating a large pericentric inversion of chromosome 18, inv(18)(p11.22q23). Individuals heterozygous for the nonrecombinant inversion were unaffected. ... Prontera et al. (2010) reported a pericentric inversion inv(18)(p11.32q22) and its recombinants in a 3-generation family, in which a mother and son carried the recombinant dup(18q)/del(18p).
-
Sarcoma, Synovial
OMIM
In 4 of the tumors, the translocation t(X;18)(p11.2;q11.2) was reciprocal. The 2 other tumors had complex translocations, which, however, always involved chromosomes X and 18 at the 2 sites mentioned. The X;18 translocation was not detected in other histologic types of soft tissue sarcoma. ... Smith et al. (1987) identified the translocation t(X;18)(p11.2;q11.2) in every cell analyzed from each of 3 synovial sarcomas. Karakousis et al. (1987) found a specific translocation between the X chromosome and chromosome 18 in 6 cases of synovial sarcoma. Wang-Wuu et al. (1987) likewise found t(X;18) in a case of synovial sarcoma. ... Knight et al. (1989) noted that the oncogene ARAF1 is not directly involved in the X;18 translocation. Miozzo et al. (1992) reported the instructive case of a patient with the Turner syndrome in whom the only X chromosome was involved in a translocation of typical form: t(X;18)(p11;q11).SSX1, SSX2, SS18, BCL2, SHCBP1, VIM, TLE1, SYT1, CD38, SSX2B, SMARCB1, CTAG1A, CTNNB1, CTAG1B, TP53, ERBB2, EWSR1, KIT, CD99, EGFR, FZD10, SSX4, CD34, CCND1, BCOR, PROM1, CTSS, IGF2, MET, PDGFRA, TNF, EZH2, HEATR3, SS18L1, CDKN2A, VEGFA, IGF1R, IGF1, IL1B, MDM2, FOXM1, MMP2, MUC1, SOX2, HGF, STAT3, CDH1, PAX8, PRKAR1A, SPG7, CXCL12, SALL2, TGFB1, SOX10, IL17A, MAPK3, RASSF1, MAPK1, HPSE, TNFSF13B, BANF1, NME1, CXCR4, ABCB1, TRIM13, PAX3, OAT, NR1I3, PRAME, MKI67, YBX1, HDAC9, MMP9, ABCC1, VCAM1, H3P10, IL10, CD274, CRK, ATF2, CXADR, ELF3, ANKRD36B, CASR, ZNF654, F5, MIR206, CXADRP1, ETFA, HBA2, ARR3, HBG1, PWWP3B, MIR145, MIR10B, ERVW-4, GDF6, KLHL34, FRMPD2, EZR, STAT6, KCNH8, MIR761, AIMP2, NR4A3, SRC, MLLT10, LOC110806263, HMGA2, CCNB3, MIR155, SYCP1, TRBV20OR9-2, MIR92B, SYP, MIR495, ADAM17, TAGLN, TAP1, TAZ, TFPI, TLR3, MIR183, FRMPD2B, CDR3, DUX4, THAS, THBD, MIR17, HBHR, RNF19A, NCOA3, SSX3, CIB1, CXCL13, AHSA1, DYM, NES, NANS, FXYD5, PIAS4, SS18L2, PUF60, FLVCR1, SIRT2, PPRC1, CIC, NUPR1, SIRT1, POLDIP2, KCNH4, NGDN, MSLN, SLC12A9, KDM2B, KIDINS220, AXIN2, TNFSF13, SMUG1, LBH, VTCN1, BRD9, RASAL3, MBD2, USP6, REPS2, TSPYL2, VAMP3, ADIPOQ, GRAP2, PRM3, PDZD4, PIEZO1, MIB1, GINS1, SNAP23, ALB, SNAI1, ELK1, EP300, EPHB2, ERCC5, ERG, ESR1, F2, F2RL1, FGFR2, FOXO1, FOLH1, GAB1, GLB1, GLO1, GSK3B, HBA1, HBB, HBG2, HLA-A, HLA-C, HMGA1, ICAM1, IFNG, IL1A, IL5, IL6, CXCL8, IDO1, ENO2, EGR1, SMN2, DUSP6, ALK, APC, AQP8, FASLG, AQP5, AQP9, ATR, ATRX, BCL6, BCR, CFB, BIK, BMP6, CAV1, CD68, CDK4, CDK9, CDKN1A, CDKN1B, CDKN3, CLDN7, CRABP1, MAPK14, CSK, CTLA4, ACE, DECR1, INHA, ITGB2, KRT7, KRT19, PIK3CG, PLK1, PLS3, PMCH, MED1, MAPK8, ALDH1A1, PTEN, PTGS2, PTN, PTPN1, RAC1, RAD23B, RBBP8, RBP4, RPL34, S100A4, SAI1, TSPAN31, CX3CL1, SELE, SLC3A1, SLC6A4, SLC12A3, SMARCA1, SMARCA2, SMN1, PIK3CD, PIK3CB, PIK3CA, MSH3, LBR, MAGEA1, MAGEA4, MB, MCM7, MDK, MDM4, MIF, CXCL9, MLH1, MMP3, MMP14, MTHFR, PDGFRB, MUC4, MYCN, NEDD4, NFKB1, NKX2-2, TBC1D25, PAEP, PAX2, PAX7, PC, PCNA, PDCD1, MAP2K7

-
Autosomal Recessive Spastic Paraplegia Type 18
Orphanet
Autosomal recessive spastic paraplegia type 18 (SPG18) is a rare, complex type of hereditary spastic paraplegia characterized by progressive spastic paraplegia (presenting in early childhood) associated with delayed motor development, severe intellectual disability and joint contractures.
-
Long Covid
Wikipedia
National Institute for Health and Care Excellence . 18 December 2020 . Retrieved 18 December 2020 . ^ a b c d e f g h i j Greenhalgh T, Knight M, A'Court C, Buxton M, Husain L (August 2020). ... National Institute for Health and Care Excellence . 18 December 2020 . Retrieved 18 December 2020 . ^ a b c d "Living with Covid19. ... Pulse Today . 6 July 2020 . Retrieved 18 October 2020 . Wise J (July 2020). ... The Independent . Retrieved 18 October 2020 . Tapper J (13 September 2020). ... Sky News . Retrieved 18 October 2020 . Hutchison C (16 October 2020).

-
Familial Hyperaldosteronism
Orphanet
Familial hyperaldosteronism (FH) is the heritable form of primary aldosteronism (PA) which comprises three identified subtypes to date: FH type I (FH-I; see this term) characterized by early-onset hypertension, glucocorticoid remediable adrenocorticotropic hormone (ACTH)-dependent hyperaldosteronism, variable hypokalemia, and overproduction of 18-oxocortisol and 18-hydroxycortisol; FH type II (FH-II; see this term) characterized by hypertension of varying severity and hyperaldosteronism not suppressible by dexamethasone; and FH type III (FH-III; see this term) characterized by profound hypokalemia, early-onset severe hypertension, non glucocorticoid-remediable hyperaldosteronism, and overproduction of 18-oxocortisol and 18-hydroxycortisol.
-
Windburn
Wikipedia
Cancer Council Australia . Retrieved 18 August 2013 . You can get burnt on windy, cloudy and cool days. ... Government of Western Australia . 7 October 2009 . Retrieved 18 August 2013 . The wind may dry the skin but does not burn it. ... Meteorological Service of New Zealand Limited . Retrieved 18 August 2013 . “I got windburnt today.” ... Time Inc. 12 October 1936 . Retrieved 18 August 2013 . ...was the first demonstration that "windburn" is really sunburn ^ "Windburn" . ... Discovery Communications . Retrieved 18 August 2013 .
-
Leptospirosis
Wikipedia
These findings are consistent with aseptic meningitis . [18] Serological tests [ edit ] Rapid detection of Leptospira can be done by quantifying the IgM antibodies using ELISA . ... During the acute phase of the disease, MAT is not specific in detecting a serotype of Leptospira because of cross-reactivity between the serovars. [18] In the convalescent phase, MAT is more specific in detecting the serovar types. [18] MAT requires a panel of live antigens and requires laborious work. [22] Molecular tests [ edit ] Leptospira DNA can be amplified by using polymerase chain reaction (PCR) from serum, urine, aqueous humour , CSF, and autopsy specimens. [18] PCR can detect Leptospira DNA in blood even before the antibody response develops. ... This disease was later known to be caused by leptospirosis. [18] By the 1950s, the number of serovars that infected various mammals had expanded significantly. ... Current Opinion in Infectious Diseases . 18 (5): 376–86. doi : 10.1097/01.qco.0000178824.05715.2c . ... "A first report of leptospirosis after liver transplantation". Transplant Infectious Disease . 18 (1): 137–40. doi : 10.1111/tid.12490 .ACHE, ADA, BCHE, MAT1A, ACAT1, TLR2, IL1B, TNF, CXCL8, ANK1, HAP1, CCL2, SPTB, IL10, TLR1, CCL3, TCOF1, SELE, S100B, S100A1, REN, TLR4, SERPINA3, TTR, TYRP1, MME, SCRN1, CADM1, SUMF2, SLCO1B3, IL22, NOD2, WDR26, ELMOD3, LRG1, CST9, PHETA1, CLYBL, VDAC1, LAMB1, MICE, LGALS3, APEX1, APOA1, AZU1, CASP3, CD40LG, CES1, CISH, CRP, F10, FUT4, GEM, CXCR3, CXCL1, CXCL2, HLA-DQB1, HLA-DRB1, HP, HSPD1, ICAM1, IL6, CXCR2, IL12RB1, IL17A, IL18, ITGAM, KIR3DL1, LBP, SLCO1B7

-
Proximal 18q Deletion Syndrome
MedlinePlus
Proximal 18q deletion syndrome is a chromosomal condition that occurs when a piece of the long (q) arm of chromosome 18 is missing. The term "proximal" means that the missing piece occurs near the center of the chromosome. ... Frequency Deletions from the q arm of chromosome 18 occur in an estimated 1 in 55,000 newborns worldwide. ... Causes Proximal 18q deletion syndrome is caused by a deletion of genetic material from one copy of chromosome 18. The deletion occurs near the middle of the q arm of the chromosome, typically in an area between regions called 18q11.2 and 18q21.2. ... Learn more about the chromosome associated with Proximal 18q deletion syndrome chromosome 18 Inheritance Pattern Proximal 18q deletion syndrome is considered to be an autosomal dominant condition. This means that a deletion in one of the two copies of chromosome 18 in each cell is sufficient to cause the disorder's characteristic features.

-
Spinocerebellar Ataxia Type 18
Orphanet
Spinocerebellar ataxia type 18 (SCA18) is a very rare subtype of type I autosomal dominant cerebellar ataxia (ADCA type I; see this term).
-
Bleeding Disorder, Platelet-Type, 18
OMIM
A number sign (#) is used with this entry because of evidence that platelet-type bleeding disorder-18 (BDPLT18) is caused by homozygous mutation in the RASGRP2 gene (605577) on chromosome 11q13. ... The patients developed mucocutaneous bleeding around 18 months of age. Features included epistaxis, hematomas, bleeding after tooth extraction, and menorrhagia.
-
Epileptic Encephalopathy, Early Infantile, 18
OMIM
A number sign (#) is used with this entry because of evidence that early infantile epileptic encephalopathy-18 (EIEE18) is caused by homozygous or compound heterozygous mutation in the SZT2 gene (615463) on chromosome 1p34. Description Early infantile epileptic encephalopathy-18 is a severe autosomal recessive neurologic disorder characterized by lack of psychomotor development apparent from birth, dysmorphic facial features, early onset of refractory seizures, and thick corpus callosum and persistent cavum septum pellucidum on brain imaging (summary by Basel-Vanagaite et al., 2013). ... Molecular Genetics In 2 unrelated patients with early infantile epileptic encephalopathy-18, Basel-Vanagaite et al. (2013) identified biallelic truncating mutations in the SZT2 gene (615463.0001-615463.0003).
-
Prelingual Deafness
Wikipedia
Centers for Disease Control and Prevention . Retrieved 2020-03-18 . ^ "Speech and Language Developmental Milestones" . NIDCD . 2015-08-18 . Retrieved 2020-03-18 . ^ CDC (2017-10-23). ... ASHA . Retrieved 18 March 2020 . ^ Duman, Duygu; Tekin, Mustafa (2012-06-01). ... American Speech-Language-Hearing Association . Retrieved 2020-03-18 . ^ "Deafness and hearing loss" . www.who.int . Retrieved 2020-03-18 . ^ a b c Gleason JB, Ratner NB (2009).
-
Human Papillomavirus Type 18 Integration Site 1
OMIM
In 2 cervical carcinoma cell lines, HeLa and C4-I, Durst et al. (1987) found that HPV18 DNA was integrated into chromosome 8, 5-prime to the MYC gene (190080). See also Couturier et al. (1991). Thus, cis-activation of cellular oncogenes seems to be responsible for malignant transformation of cervical epithelial cells in some cervical cancers.




