-
Noonan Syndrome With Multiple Lentigines
Wikipedia
In a study of 10 infants with clinical indications of NSML prior to their first birthday, 8 (80%) patients were confirmed to have the suspected mutation. ... PMC 2743116 . PMID 19467855 . ^ Coppin BD, Temple IK (1997). "Multiple lentigines syndrome (LEOPARD syndrome or progressive cardiomyopathic lentiginosis)" . ... A clinical dilemma" . J Postgrad Med . 46 (2): 98–100. PMID 11013475 . ^ Gorlin RJ, Anderson RC, Blaw M (1969). ... American Journal of Human Genetics . 78 (2): 279–90. doi : 10.1086/499925 . PMC 1380235 . ... "Noonan syndrome with café-au-lait spots and multiple lentigines syndrome are not linked to the neurofibromatosis type 1 locus". Clin. Genet . 48 (2): 85–9. doi : 10.1111/j.1399-0004.1995.tb04061.x .PTPN11, RAF1, BRAF, MAP2K1, SOS1, PTEN, KRAS, HRAS, SHOC2, EPHA2, SOS2, RRAS, RIT1, LZTR1, RASA2, RASA1, NRAS, PPP1R13L, MRAS, MAP2K2, PPP1CB, A2ML1, AKT1, MAPK3, MTOR, NF1, PIK3CG, TSC1, CDC73, TESC, SASH1, ZHX2, DSP, EGF, EPHB2, FBN1, MAPK1, FXN, SLC12A3, GAB1, IRS1, NFATC4, PIK3CA, PIK3CB, PIK3CD, MAP2K7, ACP1

-
Cytochrome P450 Oxidoreductase Deficiency
Wikipedia
PMID 32060549 . ^ Reisch N, Taylor AE, Nogueira EF, Asby DJ, Dhir V, Berry A, Krone N, Auchus RJ, Shackleton CH, Hanley NA, Arlt W (October 2019). ... PMID 31611378 . v t e Gonadal disorder Ovarian Polycystic ovary syndrome Premature ovarian failure Estrogen insensitivity syndrome Hyperthecosis Testicular Enzymatic 5α-reductase deficiency 17β-hydroxysteroid dehydrogenase deficiency aromatase excess syndrome Androgen receptor Androgen insensitivity syndrome Familial male-limited precocious puberty Partial androgen insensitivity syndrome Other Sertoli cell-only syndrome General Hypogonadism Delayed puberty Hypergonadism Precocious puberty Hypoandrogenism Hypoestrogenism Hyperandrogenism Hyperestrogenism Postorgasmic illness syndrome Cytochrome P450 oxidoreductase deficiency Cytochrome b5 deficiency Androgen-dependent condition Aromatase deficiency Complete androgen insensitivity syndrome Mild androgen insensitivity syndrome Hypergonadotropic hypogonadism Hypogonadotropic hypogonadism Fertile eunuch syndrome Estrogen-dependent condition Premature thelarche Gonadotropin insensitivity Hypergonadotropic hypergonadism v t e Inborn errors of steroid metabolism Mevalonate pathway HMG-CoA lyase deficiency Hyper-IgD syndrome Mevalonate kinase deficiency To cholesterol 7-Dehydrocholesterol path: Hydrops-ectopic calcification-moth-eaten skeletal dysplasia CHILD syndrome Conradi-Hünermann syndrome Lathosterolosis Smith–Lemli–Opitz syndrome desmosterol path: Desmosterolosis Steroids Corticosteroid (including CAH ) aldosterone : Glucocorticoid remediable aldosteronism cortisol / cortisone : CAH 17α-hydroxylase CAH 11β-hydroxylase both: CAH 3β-dehydrogenase CAH 21-hydroxylase Apparent mineralocorticoid excess syndrome/11β-dehydrogenase Sex steroid To androgens 17α-Hydroxylase deficiency 17,20-Lyase deficiency Cytochrome b 5 deficiency 3β-Hydroxysteroid dehydrogenase deficiency 17β-Hydroxysteroid dehydrogenase deficiency 5α-Reductase deficiency Pseudovaginal perineoscrotal hypospadias To estrogens Aromatase deficiency Aromatase excess syndrome Other X-linked ichthyosis Antley–Bixler syndrome This article about a disease , disorder, or medical condition is a stub .
-
Osteitis Fibrosa Cystica
Wikipedia
These instances comprise approximately 80–85% of all documented cases of hyperparathyroidism. [8] Hereditary factors Approximately 1 in 10 documented cases of hyperparathyroidism are a result of hereditary factors. ... PMID 10430265 . ^ McCance, DR; Kenny, BD; Sloan, JM; Russell, CF; Hadden, DR (1987). ... Journal of the Royal Society of Medicine . 80 (8): 505–9. doi : 10.1177/014107688708000816 . ... Mayo Clinic Proceedings . 77 (1): 87–91. doi : 10.4065/77.1.87 . PMID 11794462 . ^ Eubanks, P. ... Journal of Clinical Endocrinology & Metabolism . 91 (7): 2480–3. doi : 10.1210/jc.2005-2518 .
-
Scapular Fracture
Wikipedia
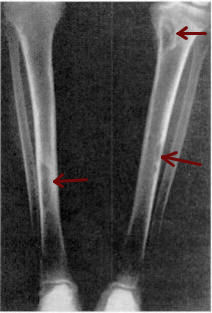
The most commonly injured areas are the scapular body, spine, neck, and glenoid rim; the scapular body or neck is injured in about 80% of cases. Fractures that occur in the body may be vertical, horizontal, or comminuted (involving multiple fragments). ... Lateral view of the left scapula Diagnosis [ edit ] X-ray showing a fracture of the clavicula and scapula Most fractures of the scapula can be seen on a chest X-ray ; however, they may be missed during examination of the film. [1] Serious associated injuries may distract from the scapular injury, [4] and diagnosis is often delayed. [3] Computed tomography may also be used. [1] Scapular fractures can be detected in the standard chest and shoulder radiographs that are given to patients who have suffered significant physical trauma , but much of the scapula is hidden by the ribs on standard chest X-rays . [4] Therefore, if scapular injury is suspected, more specific images of the scapular area can be taken. [4] Classification [ edit ] Body fractures [ edit ] Described based upon anatomic location Neck fractures [ edit ] Coracoid process fractures [ edit ] Type Description I Fracture proximal to the coracoclavicular ligament II Fracture distal to the coracoclavicular ligament Acromion fractures [ edit ] Type Description I Non- or minimally-displaced II Displaced but not affecting the subacromial space III Displacement compromising the subacromial space Glenoid fossa fractures [ edit ] Described by the Ideberg classification Treatment [ edit ] Treatment involves pain medication and immobilization at first; later, physical therapy is used. [1] Ice over the affected area may increase comfort. [6] Movement exercises are begun within at least a week of the injury; with these, fractures with little or no displacement heal without problems. [6] Over 90% of scapular fractures are not significantly displaced; therefore, most of these fractures are best managed without surgery. [3] Fractures of the scapular body with displacement may heal with malunion, but even this may not interfere with movement of the affected shoulder. [6] However, displaced fractures in the scapular processes or in the glenoid do interfere with movement in the affected shoulder if they are not realigned properly. [6] Therefore, while most scapular fractures are managed without surgery, surgical reduction is required for fractures in the neck or glenoid; otherwise motion of the shoulder may be impaired. [7] Epidemiology [ edit ] Scapular fracture is present in about 1% of cases of blunt trauma [1] and 3–5% of shoulder injuries. [4] An estimated 0.4–1% of bone fractures are scapular fractures. [2] The injury is associated with other injuries 80–90% of the time. [1] Scapular fracture is associated with pulmonary contusion more than 50% of the time. [8] Thus when the scapula is fractured, other injuries such as abdominal and chest trauma are automatically suspected. [1] People with scapular fractures often also have injuries of the ribs, lung, and shoulder. [4] Pneumothorax (an accumulation of air in the space outside the lung ), clavicle fractures , and injuries to the blood vessels are among the most commonly associated injuries. [4] The forces involved in scapular fracture can also cause tracheobronchial rupture , a tear in the airways. [9] Fractures that occur in the scapular body are the type most likely to be accompanied by other injuries; other bony and soft tissue injuries accompany these fractures 80–95% of the time. [3] Associated injuries can be serious and potentially deadly, [3] and usually it is the associated injuries, rather than the scapular fracture, that have the greatest effect on the outcome. [4] Scapular fractures can also occur by themselves; when they do, the death rate ( mortality ) is not significantly increased. [4] The mean age of people affected is 35–45 years. [2] Notes [ edit ] ^ a b c d e f g h Livingston DH, Hauser CJ (2003). ... ISBN 0-07-137069-2 . ^ a b c d e Wiedemann et al. (2000) pp. 504–507 ^ a b c d e f g Goss TP, Owens BD (2006). "Fractures of the scapula: Diagnosis and treatment".

-
Cytochrome B5 Deficiency
Wikipedia
Cytochrome b5 deficiency Specialty Endocrinology Cytochrome b 5 deficiency is a rare condition and form of isolated 17,20-lyase deficiency caused by deficiency in cytochrome b 5 , a small hemoprotein that acts as an allosteric factor to facilitate the interaction of CYP17A1 (17α-hydroxylase/17,20-lyase) with P450 oxidoreductase (POR), thereby allowing for the 17,20-lyase activity of CYP17A1. [1] [2] [3] The condition affects both adrenal and gonadal androgen biosynthesis and results in male pseudohermaphroditism . [1] The principal biological role of cytochrome b 5 is reduction of methemoglobin , so cytochrome b 5 deficiency can also result in elevated methemoglobin levels and/or methemoglobinemia , similarly to deficiency of cytochrome b 5 reductase (methemoglobin reductase). [1] References [ edit ] ^ a b c Mark A. ... S2CID 221426714 . ^ "Congenital methemoglobinemia with cytochrome b5 deficiency". N. Engl. J. Med . 315 (14): 893–4. ... External links [ edit ] Online Mendelian Inheritance in Man (OMIM): 250790 – Methemoglobinemia due to deficiency of cytochrome b 5 v t e Gonadal disorder Ovarian Polycystic ovary syndrome Premature ovarian failure Estrogen insensitivity syndrome Hyperthecosis Testicular Enzymatic 5α-reductase deficiency 17β-hydroxysteroid dehydrogenase deficiency aromatase excess syndrome Androgen receptor Androgen insensitivity syndrome Familial male-limited precocious puberty Partial androgen insensitivity syndrome Other Sertoli cell-only syndrome General Hypogonadism Delayed puberty Hypergonadism Precocious puberty Hypoandrogenism Hypoestrogenism Hyperandrogenism Hyperestrogenism Postorgasmic illness syndrome Cytochrome P450 oxidoreductase deficiency Cytochrome b5 deficiency Androgen-dependent condition Aromatase deficiency Complete androgen insensitivity syndrome Mild androgen insensitivity syndrome Hypergonadotropic hypogonadism Hypogonadotropic hypogonadism Fertile eunuch syndrome Estrogen-dependent condition Premature thelarche Gonadotropin insensitivity Hypergonadotropic hypergonadism v t e Inborn errors of steroid metabolism Mevalonate pathway HMG-CoA lyase deficiency Hyper-IgD syndrome Mevalonate kinase deficiency To cholesterol 7-Dehydrocholesterol path: Hydrops-ectopic calcification-moth-eaten skeletal dysplasia CHILD syndrome Conradi-Hünermann syndrome Lathosterolosis Smith–Lemli–Opitz syndrome desmosterol path: Desmosterolosis Steroids Corticosteroid (including CAH ) aldosterone : Glucocorticoid remediable aldosteronism cortisol / cortisone : CAH 17α-hydroxylase CAH 11β-hydroxylase both: CAH 3β-dehydrogenase CAH 21-hydroxylase Apparent mineralocorticoid excess syndrome/11β-dehydrogenase Sex steroid To androgens 17α-Hydroxylase deficiency 17,20-Lyase deficiency Cytochrome b 5 deficiency 3β-Hydroxysteroid dehydrogenase deficiency 17β-Hydroxysteroid dehydrogenase deficiency 5α-Reductase deficiency Pseudovaginal perineoscrotal hypospadias To estrogens Aromatase deficiency Aromatase excess syndrome Other X-linked ichthyosis Antley–Bixler syndrome This article about a disease , disorder, or medical condition is a stub .
-
Chorionic Hematoma
Wikipedia
Obstetrics & Gynecology: July 2003 - Volume 102 - Issue 1 - p 94-100 ^ Avneesh Chhabra, MD et al. "Subchorionic Hemorrhage" [2] , Medscape. ^ Trop, Isabelle and Levine, Deborah. ... Obstetrics & Gynecology . 105 (2): 339–44. doi : 10.1097/01.AOG.0000152000.71369.bd . PMID 15684162 . S2CID 12502344 . ^ Ben-Haroush A, Yogev Y, Mashiach R, Meizner I.

-
Nance–horan Syndrome
Wikipedia
Contents 1 Presentation 2 Genetics 3 Diagnosis 4 Management 5 History 6 References 7 External links Presentation [ edit ] Dental features: [ citation needed ] small teeth in males pointed (screwdriver shaped or conical) incisors (sometimes called Hutchinson teeth) incisors with an irregulal incisal edge canines : enlarged and globular; may be dome or bud shaped with trilobed edge premolars and molars : small, round and globular; may have supernumary lobes (mulberry or lotus flower shape) widely separated teeth ( diastemma ) hypoplastic enamel dental agenesis presence of mesiodents (median incisor behind normal upper incisors) pulp chamber anomalies Facial features: [ citation needed ] anteverted pinnae long face prominent nasal bridge and nose prognathism occasionally Ophthalmic features: [ citation needed ] bilateral congenital nuclear opacities (100%) severe amblyopia nystagmus (93%) strabismus (43%) microcornea (96%) congenital glaucoma scleral staphylomas retinal cystoid degeneration microphthalmia These lead to severe visual impairment in affected males. Other: The fourth metacarpal may be shortened 30% of patients also have some degree of intellectual impairment: of these 80% are mildly to moderately affected: the other 20% may have developmental delays and behavior problems. [ citation needed ] Carrier females display milder variable symptoms of disease. Ocular signs are present in 90% of heterozygous females. These are typically lens opacities often involving the posterior Y sutures. More rarely dental anomalies and the characteristic facial features may also occur. [ citation needed ] Genetics [ edit ] This syndrome is due to mutations in the Nance Horan gene ( NHS ) which is located on the short arm of the X chromosome (Xp22.13). [3] Diagnosis [ edit ] This section is empty. You can help by adding to it . ( August 2017 ) Management [ edit ] There is no known cure for this syndrome. ... Journal of Paediatrics and Child Health . 10 (2): 98–102. doi : 10.1111/j.1440-1754.1974.tb01098.x . ^ Nance, WE; Warburg, M; Bixler, D; Helveston, EM (1974).

-
Lateral Periodontal Cyst
Wikipedia
Journal of Oral & Maxillofacial Research . 1 (4): e5. doi : 10.5037/jomr.2010.1405 . PMC 3886068 .
-
Developmental Verbal Dyspraxia
Wikipedia
American Speech-Language-Hearing Association (ASHA) Ad Hoc Committee on Apraxia of Speech in Children (2007) [7] There are three significant features that differentiate DVD/CAS from other childhood speech sound disorders. ... "The distinct and overlapping phenotypic spectra of FOXP1 and FOXP2 in cognitive disorders" . Human Genetics . 131 (11): 1687–98. doi : 10.1007/s00439-012-1193-z . ... American Journal of Human Genetics . 76 (6): 1074–80. doi : 10.1086/430841 . PMC 1196445 . ... "V1.3) Regulation of Human Cerebral Cortical Folding and Oral Motor Development" . Neuron . 99 (5): 905–913.e7. doi : 10.1016/j.neuron.2018.07.052 .FOXP2, BCL11A, ZGRF1, CSE1L, TMX2-CTNND1, CTNND1, BCAR1, FOXP1, CRP, MMP12, MMP3, CCL2, TP53, TNF, TIMP4, TRBV20OR9-2, SHBG, NLRP3, PSD, VCP, PRKCI, PON1, PLXNA2, PECAM1, TXN, IL1R2, XDH, MIR145, APLN, SELENBP1, NOS3, MYL9, ERC1, POT1, CNTNAP2, LINC01672, B3GAT1, GAL, CCR2, MIR383, CCHCR1, NUCB2, SERPINA3, NDP, FCGR3B, FASN, EDN1, ACE, CYLD, CTNNB1, CST3, CHRNA4, CHI3L1, CTSC, CD34, CD28, CAV1, CASP1, APOE, APOB, FCGR3A, GALT, MYLK, HTC2, ALDH2, MTHFR, MMP9, MMP2, LRP1, LPA, LGALS1, LCN2, KLK1, KIT, IL18, CXCR2, CXCL8, IL6, IL1B, MYL2

-
Wilms' Tumor
Wikipedia
Treatment/prognosis [ edit ] The overall 5-year survival is estimated to be approximately 90%, [19] [20] but for individuals the prognosis is highly dependent on individual staging and treatment . ... Stage [23] Histopathology [23] 4 Year relapse-free survival (RFS) or event-free survival (EFS) [23] 4 Year overall survival (OS) [23] Treatment [23] Stage I [23] Favorable histology in children younger than 24 months or tumor weight less than 550g 85% 98% Surgery only (should be done only within the context of a clinical trial) Favorable histology in children older than 24 months or tumor weight more than 550g 94% RFS 98% Nephrectomy + lymph node sampling followed by regimen EE-4A Diffuse anaplastic 68% EFS 80% Nephrectomy + lymph node sampling followed by regimen EE-4A and radiotherapy Stage II [23] Favorable histology 86% RFS 98% Nephrectomy + lymph node sampling followed by regimen EE-4A Focal anaplastic 80% EFS 80% Nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen DD-4A Diffuse anaplastic 83% EFS 82% Nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen I Stage III [23] Favorable histology 87% RFS 94% Nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen DD-4A Focal anaplastic 88% RFS 100% (8 people in study) Nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen DD-4A Focal anaplastic (preoperative treatment) 71% RFS 71% Preoperative treatment with regimen DD-4A followed by nephrectomy + lymph node sampling and abdominal radiotherapy Diffuse anaplastic 46% EFS 53% Preoperative treatment with regimen I followed by nephrectomy + lymph node sampling and abdominal radiotherapy Diffuse anaplastic 65% EFS 67% Immediate nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen I Stage IV [23] Favorable histology 76% RFS 86% Nephrectomy + lymph node sampling, followed by abdominal radiotherapy, bilateral pulmonary radiotherapy, and regimen DD-4A Focal anaplastic 61% EFS 72% Nephrectomy + lymph node sampling, followed by abdominal radiotherapy, bilateral pulmonary radiotherapy, and regimen DD-4A Diffuse anaplastic 33% EFS 33% Immediate nephrectomy + lymph node sampling followed by abdominal radiotherapy, whole-lung radiotherapy, and regimen I Diffuse anaplastic (preoperative treatment) 31% EFS 44% Preoperative treatment with regimen I followed by nephrectomy + lymph node sampling followed by abdominal radiotherapy, whole-lung radiotherapy Stage V [23] Overall 61% EFS 80% Favorable histology 65% 87% Preoperative treatment with regimen DD-4A , followed by nephron sparing surgery or nephrecomy, staging of tumors, and chemotherapy and/or radiotherapy based on pathology and staging Focal anaplastic 76% 88% Preoperative treatment with regimen DD-4A , followed by nephron sparing surgery or nephrecomy, staging of tumors, and chemotherapy and/or radiotherapy based on pathology and staging Diffuse anaplastic 25% 42% Preoperative treatment with regimen DD-4A , followed by nephron sparing surgery or nephrecomy, staging of tumors, and chemotherapy and/or radiotherapy based on pathology and staging In case of relapse of Wilms' tumor, the 4-year survival rate for children with a standard-risk has been estimated to be 80%. [24] Epidemiology [ edit ] Wilms tumor is the most common malignant renal tumor in children. [25] There are a number of rare genetic syndromes that have been linked to an increased risk of developing Wilms Tumor. [26] Screening guidelines vary between countries; however health care professionals are recommending regular ultrasound screening for people with associated genetic syndromes. [26] Wilms' tumor affects approximately one person per 10,000 worldwide before the age of 15 years. [27] People of African descent may have slightly higher rates of Wilms' tumor. [27] The peak age of Wilms' tumor is 3 to 4 years and most cases occur before the age of 10 years. [28] A genetic predisposition to Wilms' tumor in individuals with aniridia has been established, due to deletions in the p13 band on chromosome 11. [29] History [ edit ] Dr. ... Cell . 60 (3): 509–20. doi : 10.1016/0092-8674(90)90601-A . PMID 2154335 . S2CID 29092372 . ^ Huff V (October 1998). ... PMID 7680412 . ^ Breslow NE, Beckwith JB, Perlman EJ, Reeve AE (September 2006). "Age distributions, birth weights, nephrogenic rests, and heterogeneity in the pathogenesis of Wilms tumor" .GPC3, WT1, BRCA2, DICER1, H19, TRIP13, TRIM28, REST, VHL, TP53, IGF2, CDKN1C, DIS3L2, POU6F2, AMER1, MYCN, GPC4, CTNNB1, SIX2, CTCF, DROSHA, DGCR8, ASXL1, MLLT1, SIX1, XPO5, GLIPR1, COL6A3, ARID1A, BCORL1, PALB2, BCOR, NONO, MAX, PAX2, TTN, MAP3K4, LIN28A, BMP7, PAX6, PIK3CA, NR5A1, SRY, KCNQ1OT1, PTCH1, NR0B1, KCNQ1, WWOX, ZFPM2, BUB1B, TRIM37, H19-ICR, CDC73, MAP3K1, CHEK2, NHS, DLG2, SOX9, HDAC4, VAMP7, ERBB2, TCN2, EWSR1, EXT2, HLA-A, PAX8, FLT3, GATA4, CEP57, ABL1, BUB3, WT1-AS, PCSK9, SETBP1, BCL2, NSD1, ALX4, CAT, DMRT3, DEL11P13, BUB1, PHF21A, CD34, LINC01194, ABCB1, KTWS, IGF1R, WT4, NCAM1, EGFR, NPM1, MIR193A, KRAS, IGF1, STAT3, TBC1D9, RUNX1T1, VEGFA, EGR1, PTEN, BRCA1, MTTP, HRAS, KIT, BCR, AKT1, CITED1, BDNF, VIM, AR, DES, HSPA4, TP73, EMG1, PIK3CB, PODXL, PIK3CD, SYNPO, CCN2, MDK, KMT2A, PIK3CG, RUNX1, NPHS2, IFNG, ESR1, APC, REN, PRDM2, RPL10, RARA, RBBP7, RET, PLXNA1, STIM1, NES, CDH1, HTC2, PMEL, RRM1, PTGS2, MYH11, CDKN2A, HGF, PHOX2B, CCN3, CYP19A1, RASSF1, ARHGAP24, MUC16, AMH, TOP2A, MEG3, SLC22A18, NFE2L2, NRAS, IH, PCNA, DEL11P13, PRTN3, NOTCH1, MIR483, PDGFA, MAPK3, ABCB4, PRKCA, LINC00673, MIR361, PRAME, MIR21, MVP, TP63, PROM1, MIB1, HACE1, MAPK8IP1, CTR9, SALL4, EFS, RPE65, CIB2, TET2, WNT4, CKAP4, IGF2-AS, IL22, CD274, RECK, FZD7, HMGA2, BAALC, SCT, ACTN4, MIR15A, MIR140, STAT1, LIN28B, MAP3K7, TRBV20OR9-2, TGFA, TGFB1, NKX2-1, NR2C2, UVRAG, PPP1R2C, WT2, TERT, H3P10, LMO1, CASP8, GATA1, GLI1, CCND1, CEBPA, FSHB, LMX1B, SMAD4, CRABP2, CEACAM5, BRAF, CCN1, CALB2, EZH2, ALDH1A1, HIF1A, CDH11, ABCC1, MTHFR, CD14, E2F3, AFP, GATA2, JAG1, CDKN2B, AATF, BBS9, LAMP3, HAVCR1, ELP4, PAF1, FBXW8, CDK4, TES, CRLS1, CD151, IBTK, CD59, CD44, ADGRE5, HPGDS, NCKIPSD, SGSM3, HTRA2, PIAS4, CDH13, CTNNA3, CDX1, ADGRE2, NOX4, SYCP3, KRT20, SOSTDC1, SLC38A2, CDKN3, PLCE1, KLF15, MUC4, NIPBL, RAB40B, SMR3B, FRS2, BRINP1, DCC, DDX1, DNASE1, DNMT3A, BASP1, NDC80, ATN1, IRX5, SPRY1, MSLN, HDAC5, HDAC6, EGR2, RNF40, PIEZO1, EGR3, BLCAP, CYP27B1, CD2AP, CTNNA1, CHRM3, QPRT, FBXW7, CHUK, COL4A1, DTX4, ATG4B, COL11A2, NCOA6, DKK1, PHLDA1, CRP, KLHL2, USP18, CSF2, CSF3, PTP4A3, CORO1A, CSF3R, QRSL1, CBFB, CD40LG, ALK, ANXA5, MIR370, MIAT, MIR23A, MIR215, APRT, MIR204, MIR203A, MIR200C, MIR19B1, MIR199B, MIR195, KLK3, MIR192, MIR16-1, FASLG, MIR155, MIR144, MIR141, MIR429, SNHG6, PCDHA@, LINC00273, H3P47, LINP1, ACVR2B, ADAR, APOBEC3A_B, PARP1, SOX21-AS1, MIR1180, MIR1270, CD24, LINC00893, MIR190B, RNA18SN5, MIR613, MIR600, MIR590, MIR572, MIR562, MIR539, AREG, MIR130B, ATF3, C17orf97, BMPR1A, CMIP, WLS, TSPO, CA9, CALCA, IRX3, MARCKSL1, CALR, CASP3, IL21, RUNX3, WFDC1, SEMA6A, ENO2, CD80, INTS2, CD38, PNPLA2, PRAM1, DLGAP1-AS2, C19orf48, CLYBL, BAK1, PWAR4, SOX2-OT, LUZP2, BARD1, NAPSB, AMER2, APOBEC3A, BCL2A1, KRT88P, OPN1SW, OSR1, BCS1L, WTIP, SAT2, BMP2, MTDH, LINC00473, EPHA2, KLF4, RGS6, IL17A, RBP2, INSR, RB1, ITGAX, RAP1A, PTPRC, PTN, JAK2, PTH, KDR, KRT7, LAMB2, PRM1, LHCGR, LHX1, PTPA, PPP2R1A, PPBP, PON1, INS, IL15, LMO2, RFC1, SLC5A5, SMTN, SLC2A3, SLC2A1, SIX3, IFI16, STIL, IFNB1, SHMT1, SRSF1, IGF2R, SET, SALL1, SALL2, S100A4, IL2, IL4, IL6, RGS4, PMS2, PLCG2, RIN1, SERPINE1, OGG1, ROR1, MKI67, MLH1, NPHS1, NPHP1, MPZ, NPY, MRC1, NNAT, NKX6-1, MSH3, NGFR, NGF, MSX1, NF2, NEFL, NAP1L4, MYOD1, MIP, PAWR, PLAG1, CD99, PKHD1, PIK3R1, LSAMP, SMAD2, PHF2, PHB, MCM2, MDM4, PGR, PFN1, SERPINF1, PECAM1, PDGFRB, MEIS1, MET, PBX2, MFAP1, PAX5, PAX3, SLC8A1, SLC19A1, SNAI2, FEN1, FZD1, BAP1, FGF8, MIA, FH, WT3, FLI1, FXR1, RASSF7, DEK, FZD5, CXCR4, FLII, FN1, ZNF224, ZBTB16, FUT4, GABPA, WNT5A, FGF3, MKNK1, SMARCB1, FANCB, VPS4B, EPHB2, ERCC2, MUC1, S1PR2, ETS1, FIBP, ARHGEF1, F2RL3, RTL8C, EYA1, CCNA1, HDAC3, CFLAR, DLK1, RNMT, MBTPS1, BECN1, AKR1C3, GAPDH, VDR, GDNF, TTK, HNRNPL, HNF1B, HNF1A, TBXA2R, TAL1, HOXB4, HOXD10, STK11, HSPA1A, HSPA1B, HSP90AA1, HSP90AA2P, SRPK1, SRF, SRD5A2, SPP1, SPI1, IRF8, SOD1, HLA-DQA1, TERF1, TERF2, TSPAN7, TTF1, PHLDA2, TSG101, TSC2, GLRA2, MSH6, GUSB, HBB, HCRTR1, HLA-C, TIMP4, TIMP1, THY1, THOP1, THBS1, THBD, TH, HDAC1, SFRP1

-
Flail Chest
Wikipedia
Breathing exercises will also include coughing procedures. [15] Furthermore, range of motion exercises are given to reduce the atrophy of the musculature. [16] With progression, resistance exercises are added to the regimen to the shoulder and arm of the side containing the injury. ... "Management of rib fractures in traumatic flail chest: a meta-analysis of randomised controlled trials". The Bone & Joint Journal . 98-B (8): 1119–25. doi : 10.1302/0301-620x.98b8.37282 . ... "Flail Chest in a Neonate Resulting from Nonaccidental Trauma". Southern Medical Journal . 99 (5): 536–538. doi : 10.1097/01.smj.0000216471.54786.e5 . ^ Granetzny A; Abd El-Aal, M; Emam, E; Shalaby, A; Boseila, A (2005).

-
Oneiroid Syndrome
Wikipedia
Общая психопатология: Учебное пособие для студентов высших учебных заведений [ General psychopathology: Textbook for students of higher educational institutions ] (in Russian). Moscow: Academia. pp. 80–82. ISBN 5-7695-0838-8 . ^ a b Kaptsan, A; Miodownick, C; Lerner, V (2000). ... The Israel Journal of Psychiatry and Related Sciences . 37 (4): 278–85. PMID 11201932 . ^ a b Shorter, E. (2005). ... Journal of Psychiatry & Neuroscience . Joule Inc. 35 (4): E5–6. doi : 10.1503/jpn.100087 . ISSN 1180-4882 .
-
Cushing's Disease
Wikipedia
Pituitary adenomas are responsible for 80% of endogenous Cushing's syndrome, [3] when excluding Cushing's syndrome from exogenously administered corticosteroids . ... Considering this impact, the name of Itsenko was added to the title in some East European and Asian countries, and the disease is called Itsenko-Kushing disease. [ citation needed ] References [ edit ] ^ "Whonamedit – Nikolai Mikhailovich Itsenko" . ... "Treatment of adrenocorticotropin-dependent Cushing's syndrome: a consensus statement" . J Clin Endocrinol Metab . 93 (7): 2454–2462. doi : 10.1210/jc.2007-2734 . ... "Efficacy of medical treatment in Cushing's disease: a systematic review" . Clinical Endocrinology . 80 (1): 1–12. doi : 10.1111/cen.12345 . ... "National trends, complications, and outcomes following transsphenoidal surgery for Cushing's disease from 1993 to 2002". Neurosurgical Focus . 23 (3): E7. doi : 10.3171/foc.2007.23.3.9 . PMID 17961019 .CRH, POMC, PRKAR1A, PRKACB, NR3C1, USP8, CDH23, GABRA6, DRD2, CYBB, SERPINA1, GIPR, PRKACA, GIP, ARMC5, CYP11B1, PDE11A, VWF, HSD11B1, MEN1, CYP17A1, GNAS, SST, CGB3, CGA, HSD11B2, HTC2, REN, CGB5, CGB8, PDE8B, CTNNB1, MC2R, GH1, GHRL, SULT2A1, IL6, FDXR, RNU1-4, PRL, LEP, LHCGR, TP53, NR3C2, AGT, DST, TXNIP, AKR1B1, RNU1-1, BDNF, PHLDA2, LGR6, NDRG2, GBA3, SLC25A19, PPARG, BRD2, POR, COASY, FBXO32, RET, BCOR, TWIST1, SLC8A1, KRT20, SOST, SLC12A3, SMUG1, PMPCA, UTS2, C1QL1, HDAC9, BEST1, STAR, TXN, CCDC6, SERPINA3, PECAM1, TSC22D3, ACE, CYP11B2, CYP3A4, CYB5A, CPA1, COX8A, CNC2, CETP, SCARB1, SERPINA6, CAMP, CACNA1D, BGLAP, AVP, ATR, APRT, AGTR2, AGTR1, AGRP, ADRA2A, ACP5, DMD, E2F1, MFAP1, F2, CYP4F3, KRT5, KCNJ5, IRF6, IL18, CXCL8, ACAT1, IGF2, IGF1R, IGF1, HTR4, GSTA1, GHSR, FOLH1, FOXO3, FKBP5, FH, FDX1, FASN, F12, F5, PGR-AS1
-
Obesity In Sweden
Wikipedia
Sweden is the 90th fattest country in the world. [1] In 2009, the number of people who are considered overweight or obese had not increased for the first time in 70 years. [2] Claude Marcus , a leading Swedish nutrition expert from the Karolinska Institutet , stated that one solution is to introduce a fat tax . [3] Folksam refused to insure a 5-year-old girl from Orust . [4] The insurance company refused her insurance based on "serious overweight/obesity". [4] A report showed that children whose parents were better educated had a lower chance of becoming overweight. [5] Contents 1 Cause 2 Effects 3 Programs 4 Forbes ranking 2007 5 References Cause [ edit ] Lack of exercise along with sugar-sweetened foods and drinks have caused one out of six five-year-olds in Sweden to be overweight or obese. [5] The breakdown is 12.9% of children are considered overweight and 4.3% are considered obese . [5] Effects [ edit ] Several studies have shown that obese men tend to have a lower sperm count , fewer rapidly mobile sperm and fewer progressively motile sperm compared to normal-weight men. [6] Programs [ edit ] School nurses in Uppsala , Uppsala County will be prescribing exercise to teenage boys. [7] The prescribed exercise can be anything from participating in a sport to walking. [7] Spaces will be available for the participants. [7] Forbes ranking 2007 [ edit ] Source : Forbes.com [1] Ranking Country Percentage Overweight 85 Panama 51.4 86 Tunisia 51.0 87 Saint Vincent and the Grenadines 50.6 88 Brazil 50.5 89 Belize 49.8 90 Sweden 49.7 91 Norway 49.1 92 Russia 49.1 93 El Salvador 48.7 94 Lesotho 48.5 95 Suriname 47.8 References [ edit ] ^ a b "World's Fattest Countries" .
-
Cole-Carpenter Syndrome
Wikipedia
It is made by sequencing the P4HB, SEC24D and CRTAP genes. [ citation needed ] Differential diagnosis [ edit ] Pfeiffer syndrome Osteogenesis imperfecta Osteoglophonic dwarfism Treatment [ edit ] There is no specific treatment for this condition currently known and management of its various features is the norm. [ citation needed ] History [ edit ] This condition was first described in 1987. [1] References [ edit ] ^ a b Cole DEC, Carpenter, TO (1987) Bone fragility, craniosynostosis, ocular proptosis, hydrocephalus, and distinctive facial features: a newly recognized type of osteogenesis imperfecta. J Pediat 110: 76-80 ^ Rauch F, Fahiminiya S, Majewski J, Carrot-Zhang J, Boudko S, Glorieux F, Mort JS, Bächinger HP, Moffatt P (2015) Cole-Carpenter syndrome is caused by a heterozygous missense mutation in P4HB. ... Epub 2015 Feb 12. ^ Balasubramanian M, Pollitt RC, Chandler KE, Mughal MZ, Parker MJ, Dalton A, Arundel P, Offiah AC, Bishop NJ (2015) CRTAP mutation in a patient with Cole-Carpenter syndrome. Am J Med Genet A 167A(3):587-91. doi: 10.1002/ajmg.a.36916 Classification D OMIM : 112240 MeSH : C535963 C535963, C535963

-
Essential Thrombocythemia
Wikipedia
All mutations (insertions or deletions) affected the last exon, generating a reading frame shift of the resulting protein, that creates a novel terminal peptide and causes a loss of endoplasmic reticulum KDEL retention signal . [6] [7] Diagnosis [ edit ] The following revised diagnostic criteria for essential thrombocythemia were proposed in 2005. [8] The diagnosis requires the presence of both A criteria together with B3 to B6, or of criterion A1 together with B1 to B6. [9] The criteria are as follows: [9] A1. ... No evidence of iron deficiency stainable iron in the bone marrow or normal red cell mean corpuscular volume B3. No evidence of polycythemia vera hematocrit < midpoint of normal range or normal red cell mass in presence of normal iron stores B4. ... Patients with the Philadelphia chromosome have a potential for the development of acute leukemia, especially acute lymphocytic leukemia . B5. No evidence of myelofibrosis no collagen fibrosis and ≤ grade 2 reticulin fibrosis (using 0–4 scale) B6. ... Internal and Emergency Medicine . 5 (3): 177–84. doi : 10.1007/s11739-009-0319-3 . ... The New England Journal of Medicine . 369 (25): 2379–90. doi : 10.1056/NEJMoa1311347 . PMID 24325356 .JAK2, CALR, SH2B3, MPL, THPO, IFNA2, TET2, TP53, TGFB1, PDGFA, FGF2, PDGFB, MYB, BCR, ABL1, CD34, CD177, ASXL1, PRB1, SOAT1, EPO, IFNA13, IFNA1, STAT5A, IDH2, STAT5B, VEGFA, LINC01152, AR, SRSF2, GATA1, F5, F2, SELP, IDH1, STAT3, DERL1, NFE2, IL6, SOCS3, BCL2, F3, HPSE, STAT1, CXCL8, TFPI, ITGAM, ITGB3, SF3B1, KIT, PTX3, LCN2, MDM2, PGF, SELE, MMP9, TERT, MVD, MYC, NOS3, SOCS1, HMGA2, HBS1L, RN7SL263P, FLI1, CSF2, CBL, EPOR, CD63, CTNNB1, G6PD, EVPL, EZH2, BAX, CRP, CSF3R, LRPPRC, PIAS3, WDR4, HLA-B, BAK1, CHEK2, CCND1, DAAM1, MTUS2, ARSA, DKK1, HDAC9, HDAC6, NAAA, TLR4, BNIP3L, U2AF1, UCP2, BID, CXCR4, LAP, BDNF, SLC14A2, CNTNAP1, BCL2L2, DLK1, SOCS2, BCL2L1, USP14, MYOM2, GDF15, DKK3, RABGEF1, IL37, MIR146B, CYGB, ANXA5, MIR125A, MIR143, MIR203A, MIR221, MIR490, GGTLC5P, THBS1, GGTLC3, GGT2, GGTLC4P, BCL2L2-PABPN1, MIR4639, AK6, AKT1, NLRP3, MLIP, HAVCR2, PRAM1, SETD2, IL22, PTOV1, TERF2IP, ARG2, BCOR, FASLG, MTUS1, HAMP, ACE2, APOA1, HDAC11, FIP1L1, QTRT1, SESN2, CALB2, CD69, CASP9, RUNX1T1, ITGB2, FLT1, JAK1, FLII, FCGR2A, LDHA, LDHC, LGALS3, LIG3, SMAD4, MCAM, FANCB, MFGE8, ATXN3, MMP2, ITGA2B, IL10, CXCR2, IFNG, HIF1A, HFE, IFI27, SERPIND1, H2AX, CXCL1, IGF1, CXCR1, IGF2, IGH, IL3, NR3C1, IL6ST, GGT1, COX1, MTHFR, ERCC2, SELENOP, S100A9, S100A12, ACSM3, CXCL12, CHIT1, CHI3L1, AKR1C4, REN, SLC14A1, CDR1, SPP1, CDH13, HSPA4, CD14, S100A8, RARS1, EDN1, SERPINE1, NFATC2, ACE, ADM, NRAS, NTRK1, PAEP, PCNA, RAP1A, PDGFRA, CPB1, PROC, PROS1, PTGS1, CISH, NM

- Verruciform Xanthoma Wikipedia
-
Serotonin Syndrome
Wikipedia
ISBN 9781451188509 . ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa ab ac ad ae af ag ah ai aj ak al am an ao ap aq ar as at au av aw ax ay az ba bb bc bd be Boyer EW, Shannon M (March 2005). ... "The clinical toxicology of metamfetamine" . Clin Toxicol . 48 (7): 675–94. doi : 10.3109/15563650.2010.516752 . ... Arch Dis Child Fetal Neonatal Ed . 85 (2): F147–8. doi : 10.1136/fn.85.2.F145g . ... J Toxicol Clin Toxicol . 42 (3): 277–85. doi : 10.1081/CLT-120037428 . PMID 15362595 . ... J Emerg Med . 16 (4): 615–9. doi : 10.1016/S0736-4679(98)00057-2 . PMID 9696181 . ^ Gillman PK (1999).
-
Weill-Marchesani Syndrome
Orphanet
Short stature (usually below the third percentile) and brachydactyly are present in 98% of patients. Clinical description The following frequencies of ophthalmological manifestations are observed: myopia 94%, microspherophakia 84%, ectopia lentis 73%, glaucoma 80%, and cataract 23%. ... Etiology Both autosomal recessive (AR) and autosomal dominant (AD) modes of inheritance have been described. ... Heterozygous mutations within the FBN1 gene (15q21.1) have been identified in patients and are transmitted in an AD manner, giving another example of the large clinical expressivity of fibrillin-1. ... Genetic counseling Clinical homogeneity has been demonstrated despite the genetic heterogeneity in AR and AD families. However, this leads to difficulties in genetic counseling of sporadic cases.
-
Functional Gastrointestinal Disorder
Wikipedia
The current Rome IV classification, published in 2016, is as follows: [1] A. Esophageal disorders A1. Functional chest pain A2. Functional heartburn A3. ... Excessive supragastric belching B2b. Excessive gastric belching B3. Nausea and vomiting disorders B3a. ... Functional biliary sphincter of Oddi disorder E2. Functional pancreatic sphincter of Oddi disorder F. ... S2CID 6441439 . ^ "Rome Foundation // Scoring Rome III Questionnaire using SAS" . ^ Sperber AD, Drossman DA, Quigley EM (2012). "The global perspective on irritable bowel syndrome: a Rome Foundation-World Gastroenterology Organisation symposium".CSF3, NFE2L2, CHD8, MTHFR, ABCC2, EDN1, MTR, CCK, MYLK, GAST, POMC, KEAP1, AGER, LRRC8D, BARX1, CRTC1, ALDH1A2, CPE, TNF, ACAD8, NPR3, S100A8, TGFB1, CFTR, GP2, ABCB1, CNR1, CCL11, FMO3, HP, GUCY2C, IL1A, IL1B, DPP4, NOD2, VDR, VIP, RET, NR1I2, RARRES2, VIPR1, SCT, S100B, SLC6A4, SLC8A1, TSPAN8, TLR2, SPI1, TGM2, PHOX2B, TGFBR2, TFF1, CACNA1G, POLR1A, NUP155, TAAR1, HOTAIR, HULC, MIR375, MIR369, MIR26B, MIR15A, MIR155, PRSS57, GOLGA6A, SLC9C1, CARMIL2, CCDC26, RAMAC, NOD1, EHMT1, PROK2, COG6, IFT122, RCBTB1, MOCOS, MLXIPL, IL22, PSG2, TBC1D9, POLR3A, SLC26A1, RAB27A, PARP1, PRKAR1A, PPARG, GPT, GDNF, GABPA, FOXF2, FOXF1, FAAH, F2RL1, ETFA, SLC26A3, DEFB1, CTSW, CRP, COL11A2, COL1A2, CNC2, CEACAM7, CEACAM3, CEACAM5, CD34, CAT, CASR, SERPING1, TNFRSF17, ATP4A, ATP12A, APOA1, NR0B1, GUCA2B, HFE, HNF4A, MUC6, PON3, PON1, PMP22, PDGFRA, PCSK1, PAEP, AFP, NPY, CEACAM6, MYO9B, MYB, MUTYH, MUC1, HRH2, MSD, MPZ, LYZ, KRAS, ITPA, IL18, IL17A, IL15, IL10RB, IL10RA, CXCL8, IL6, CCAT1










