-
Wheat Leaf Rust
Wikipedia
This name was used by Gaeumann (1959) [4] in his comprehensive book about rust fungi of middle Europe. Mains (1933) was among the first scientists who used a species name with a broad species concept for WLR. [5] He considered P. rubigo-vera as a current name and put 32 binomials as synonyms of that species. ... Walthan, MA, USA. p. 269. ^ Huerta-Espino, J. First report of virulence to wheat with leaf rust resistance gene Lr19 in Mexico .

-
Paroxysmal Cold Hemoglobinuria
Wikipedia
Described by Julius Donath (1870–1950) and Karl Landsteiner (1868–1943) in 1904, PCH is one of the first clinical entities recognized as an autoimmune disorder . [2] Contents 1 Signs and symptoms 2 Cause 3 Pathophysiology 4 Diagnosis 4.1 Classification 5 Management 6 Epidemiology 7 See also 8 References 9 External links Signs and symptoms [ edit ] Pediatric patients usually present with acute onset of hemolytic anemia with fatigue , exercise intolerance , pallor , jaundice , and hemoglobinuria , preceded by exposure to cold temperature and preceding viral-like illness. ... Reticulocytosis may not be apparent in the acute phase or when there is viral-induced myelosuppression . [1] Once the clinical suspicion of autoimmune hemolytic anemia is made, direct antiglobulin test (DAT) or direct Coombs' test is the first line of investigation to confirm the presence of warm autoantibodies. [9] Testing with polyspecific and IgG-specific antiglobulin agents is usually negative, and that with C3-specific agent may be positive.
-
2016 Irkutsk Mass Methanol Poisoning
Wikipedia
The two alcohols are similar in many respects and cannot readily be distinguished, and their contents differed from the labels on the bottles, which indicated that they contained ethanol [1] [11] [12] —specifically, "93 percent of ethyl alcohol, hawthorn extract, lemon oil , diethyl phthalate and glycerol ". [13] An investigation later revealed that the methanol was usually used in the local production of antifreeze . [7] According to early reports on 19 December, a total of 57 people were hospitalized, with 49 dying. [1] [11] The victims were described as being poor residents of the Novo-Lenino neighborhood in Irkutsk, all between the ages of 35 and 50. [12] [14] Subsequent reports increased the number affected: first to 55 deaths (with a total of 94 affected), [15] then 62 (with 107 affected), [16] [17] 77 (number of affected not given), [18] and 78. [7] The final death toll was 74, lowered from earlier reports after it was discovered that some of the deaths were the result of drinking too much of the non-fraudulent ethanol-based bath lotion. [7] A total of 123 people were hospitalized. [7] About a third of them were found in their homes, having died before being able to call for an ambulance. [19] Of the remainder, a problem in attempting to treat them was that fomepizole , a methanol antidote , is not certified for use in Russia and is therefore not available in the country's hospitals. [2] Overall, the victims included a doctor, teachers, nurses, and drivers; The New York Times described the majority as holding "steady if low-paying jobs". [2] [19] Aftermath [ edit ] In the immediate aftermath of the poisoning, a state of emergency was declared. [7] Twenty-three people involved in the production of the lotion were arrested by Russian authorities, many of which were local vendors who sold the product, and one senior regional government official for the greater Siberian region being charged with negligence. [18] [20] About 500 litres (130 US gal) of remaining counterfeit lotion were seized from the underground facility where it had been produced, [1] and a few days later 13,500 litres (3,600 US gal) of methanol-containing liquid was seized from a warehouse in Irkutsk. [21] A further five people were arrested in January 2017, charged with selling and publicizing surrogate alcohol. [22] After the incident, a spokesperson for Russian president Vladimir Putin called it a "terrible tragedy", [1] blaming it on a failing of "supervisory bodies", [2] and added: "What happened in Irkutsk was a tremendous tragedy. ... The latter's legalization had been mooted prior to the poisoning. [7] Furthermore, the minimum legal price of vodka was lowered in both January and May 2017. [7] Individuals interviewed by a New York Times reporter in February 2017 were skeptical that any measures would be successful in significantly impacting illegal alcohol sales, given that it was such a high percentage of the total market for alcohol. [2] Indeed, vendors in Irkutsk reported that sales of surrogate alcohols did not decline after the poisoning. [7] Still, Rospotrebnadzor announced at the end of January that the country had seen its first decline in monthly alcohol poisoning deaths in five years. [29] See also [ edit ] List of methanol poisoning incidents Prohibition in the Russian Empire and the Soviet Union References [ edit ] ^ a b c d e f g h Isachenkov, Vladimir (19 December 2016).

-
Prosopamnesia
Wikipedia
Many face perception and memory tests have been developed and used by researchers in the past including the Warrington Recognition Memory for Faces, Benton Facial Recognition Test and later, The Cambridge Face Perception Test and Cambridge Face Memory Test, which were developed in order to address the shortcomings of the first two tests. [10] The Warrington Recognition Memory tests "contain abundant non-internal facial feature information" and the Benton Facial Recognition Test allows the test subject to "rely on feature matching strategies using the hairline and eyebrows rather than recognizing the facial configuration". [11] The Cambridge Face Perception Test allows participants to look at a target face, while ranking 6 other faces according to their resemblance to the target face. [12] Prosopagnosics will fail this test, while prosopamnesiacs will pass it, making it the hallmark for distinguishing between the two disorders. ... History [ edit ] Prosopamnesia was first proposed as a distinct neurological disorder in 1996. [4] Doctors observed a patient who appeared to have acquired prosopagnosia after an injury to the temporal lobe .
-
Perception Of English /r/ And /l/ By Japanese Speakers
Wikipedia
McClelland, Fiez & McCandliss (2002) argue that it is possible to train Japanese adults to distinguish speech sounds they find difficult to differentiate at first. They found that speech training results in outcomes indicating a real change in the perception of the sounds as speech, rather than simply in auditory perception. ... ", Journal of the Acoustical Society of America , 96 (4): 2076–2087, Bibcode : 1994ASAJ...96.2076L , doi : 10.1121/1.410149 , PMC 3518835 , PMID 7963022 Logan, John; Lively, Scott; Pisoni, David (1991), "Training Japanese listeners to identify English /r/ and /l/: a first report", Journal of the Acoustical Society of America , 89 (2): 874–886, Bibcode : 1991ASAJ...89..874L , doi : 10.1121/1.1894649 , PMC 3518834 , PMID 2016438 McClelland, J.L.; Fiez, J.A.; McCandliss, B.D. (2002), "Teaching the /r/-/l/ Discrimination to Japanese Adults: Behavioral and Neural Aspects", Physiology & Behavior , 77 (4–5): 657–662, doi : 10.1016/S0031-9384(02)00916-2 , PMID 12527015 Miyawaki, Miyawaki; Strange, W.; Verbrugge, R.R.; Liberman, A.M; Jenkins, J.J.; Fujimura, O. (1975), "An effect of linguistic experience: the discrimination of [r] and [l] by native speakers of Japanese and English", Perception and Psychophysics , 18 (5): 331–340, doi : 10.3758/BF03211209 Takagi, Naoyuki (1995), "Signal detection modeling of Japanese learners' /r/-/l/ labeling behavior in a one-interval identification task", Journal of the Acoustical Society of America , 97 (1): 563–574, Bibcode : 1995ASAJ...97..563T , doi : 10.1121/1.413059 , PMID 7860833 Takagi, Naoyuki; Mann, Virginia (1995), "The limits of extended naturalistic exposure on the perceptual mastery of English /r/ and /l/ by adult Japanese learners of English", Applied Psycholinguistics , 16 (4): 379–405, doi : 10.1017/S0142716400066005 Vance, T. (1987), An introduction to Japanese phonology , Albany, NY: State University of New York Press Yamada, Reiko; Tohkura, Y. (1992), "The effects of experimental variables on the perception of American English /r/ and /l/ by Japanese listeners", Perception and Psychophysics , 52 (4): 376–392, doi : 10.3758/BF03206698 , PMID 1437471 Zawadzki, P.A.; Kuehn, D.P. (1980), "A cineradiographic study of static and dynamic aspects of American English /r/", Phonetica , 37 (4): 253–266, doi : 10.1159/000259995 , PMID 7443796
-
Scrupulosity
Wikipedia
No association between OCD and depth of religious beliefs has been demonstrated, although data are scarce. [6] There are large regional differences in the percentage of OCD patients who have religious obsessions or compulsions, ranging from 0–7% in countries like the U.K. and Singapore, to 40–60% in traditional Muslim and orthodox Jewish populations. [10] History [ edit ] John Moore (shown c. 1691–1703 ) was the first to describe the disorder, calling it "religious melancholy". [11] Scrupulosity is a modern-day psychological problem that echoes a traditional use of the term scruples in a religious context, e.g. by Catholics , to mean obsessive concern with one's own sins and compulsive performance of religious devotion. [12] This use of the term dates to the 12th century. [13] Several historical and religious figures suffered from doubts of sin, and expressed their pains. Ignatius of Loyola , founder of the Jesuits , wrote "After I have trodden upon a cross formed by two straws ... there comes to me from without a thought that I have sinned ... this is probably a scruple and temptation suggested by the enemy." [10] Alphonsus Liguori , the Redemptorists ' founder, wrote of it as "groundless fear of sinning that arises from 'erroneous ideas'". [13] Although the condition was lifelong for Loyola and Liguori, [14] [15] Thérèse of Lisieux stated that she recovered from her condition after 18 months, writing "One would have to pass through this martyrdom to understand it well, and for me to express what I experienced for a year and a half would be impossible." [16] Martin Luther also suffered from obsessive doubts; in his mind, his omitting the word enim ("for") during the Eucharist was as horrible as laziness, divorce, or murdering one's parent. [17] Although historical religious figures such as Loyola, Luther and John Bunyan are commonly cited as examples of scrupulosity in modern self-help books, some of these retrospective diagnoses may be deeply ahistorical: these figures' obsession with salvation may have been excessive by modern standards, but that does not mean that it was pathological. [18] Scrupulosity's first known public description as a disorder was in 1691, by John Moore , who called it "religious melancholy" and said it made people "fear, that what they do, is so defective and unfit to be presented unto God, that he will not accept it". [11] Loyola, Liguori, the French confessor R.P.
-
Autoimmune Hypophysitis
Wikipedia
Recent research has focused on a defect at the CTLA-4 gene which, coupled with other factors, may result in autoimmunity primarily focusing on certain endocrine glands including the pituitary and thyroid. [3] Diagnosis [ edit ] Lymphocytic hypophysitis continues to be a diagnosis of exclusion, and histopathology with tissue biopsy is needed for a definitive diagnosis.[3] However, clinical, laboratory data, and imaging can all help with the diagnosis.[8] First and foremost, patients present with symptoms of hypopituitarism and must undergo pituitary hormone function evaluation. [9] Biopsy is the only means of accurate diagnosis as no autoantigen has been discovered. [8] [10] Biopsy of the pituitary gland is not easily performed with safety as it sits under the brain, however, a test does exist to detect antibodies to the pituitary without biopsy: autoantibodies to M(r) 49,000 pituitary cytosolic protein may represent markers for an immunological process affecting the pituitary gland. [3] Tests for normal pituitary gland hormone production tend to be expensive and in some cases difficult to administer. ... However, it is thought that this may be an underestimate, especially due to the recent use of immune checkpoint inhibitors for cancer treatments, which have endocrine side effects affecting the pituitary gland. [19] Although cases have been reported in children and the elderly, the mean age of diagnosis for men is 44.7 years, and the mean age of diagnosis for women is 34 years. [20] History [ edit ] Autoimmune attack of the pituitary gland resulting in reduced hormone production was first discovered as a result of an autopsy in 1962.
-
Fever
Mayo Clinic
If a seizure occurs: Lay your child on the side or stomach on the floor or ground Remove any sharp objects that are near your child Loosen tight clothing Hold your child to prevent injury Don't place anything in your child's mouth or try to stop the seizure Call 911 or your local emergency number if a seizure lasts more than five minutes or your child doesn't appear to recover well after the seizure Get emergency room or urgent care services if it's your child's first febrile seizure. If your child doesn't need emergency care, see your child's health care provider as soon as possible for further evaluation. ... What to expect from your doctor Be prepared to answer questions, such as: When did the symptoms first occur? What method did you use to take your or your child's temperature?IL6, IL1B, PTGS2, IL1RN, HTR1A, STAT3, IFNG, TNF, IL1A, MVK, CSF3, IL2, CXCL8, TNFRSF1A, HMGB1, PTGES, POMC, SOD2, HTR2A, IFNA2, PRL, CRH, FSHB, HSPB1, TPH2, NOS1, ASPG, CCK, HSF1, HMOX1, HPGD, CCN2, DRD1, A2M, EPHA3, IL6R, STAR, IL10, CBR1, CCL5, PLA2G4A, MEFV, CCR5, CNR1, VIM, TP53, NLRP3, BCL2, BRCA2, COX2, CACNA1A, TLR4, HLA-DRB1, HLA-B, CFH, NLRP1, ATP1A3, ADAMTS13, CPT2, PRNP, XIAP, EDA, CTLA4, AVP, CYBB, COX1, IL12A, CALR, HLA-DPB1, FAS, PRTN3, JAK2, WAS, EIF2B4, ANK1, TH, TCF3, EIF2B2, PTPN22, STING1, ATP1A2, SPINK1, RYR1, BCR, EIF2B1, CHEK2, XPC, SLCO1B1, BCOR, TET2, P4HTM, SCYL1, GYPC, HMBS, ADA2, MIF, GFI1, HLA-DPA1, IGH, ERAP1, MPL, IFNGR1, MST1, POMP, NOD2, ATP6, NLRC4, CFHR1, IRF8, COX3, ND1, ND2, LIPA, LBR, LIG4, IGHM, NABP1, GPC3, IL7R, IL12B, HSPA4, HSPB2, LRRC8A, DCLRE1C, IRAK1, IL2RG, BTNL2, HSP90AA1, HBB, GPR35, GLA, KCNJ1, CHD7, GPT, IGLL1, SLC29A3, KRT8, HMGCL, KRT18, NGLY1, NUMA1, ND3, SLC11A1, STAT5B, STAT4, SRP54, SPTB, SPTA1, SPP1, TCIRG1, IKZF1, SLC12A1, SLC4A1, ND4, SCNN1G, SCNN1B, SCNN1A, CFHR3, SCN1A, MALT1, RMRP, REST, POLR3A, STAT6, TCF4, MLX, TRIM28, EIF2B3, EIF2B5, BCL10, HSPB3, STX11, CASK, PSTPIP1, KLRC4, TRIP13, ZBTB16, XPA, WT1, WIPF1, TRPV1, TSC2, TSC1, LPIN2, SH2B3, HCN4, RB1, RARA, RANBP2, HTRA2, CYBC1, NPM1, NOTCH3, BLNK, NCF4, NCF2, NAB2, MYD88, TRNW, TRNV, TRNS2, TRNS1, TRNQ, TRNL1, TRNK, TRNH, TRNF, ND6, ND5, SLCO1B3, FOXP1, RAG2, PGK1, RAG1, RAB27A, TREX1, POU6F2, PTPN3, CTRC, KIF1B, LPIN1, ATP13A2, HTRA1, PRSS2, PRSS1, SMUG1, PRKAR1A, PMM2, PML, NOC2L, PIK3R1, IL36RN, GATA2, KLHL7, CACNA1S, H19, UBAC2, CD247, BIRC3, AQP2, NCF1, CD3E, ATM, CD3D, ATP7A, FBP1, EPB41, AVPR2, HAVCR2, EPB42, RUNX1, CCND1, CAT, BCL6, F5, ERCC2, ERCC3, DST, IRF2BP2, CASP3, BTK, C1QA, C1R, C4A, ERCC4, CD27, ELANE, ERCC5, GAA, G6PD, LACC1, DDB2, COL1A1, IL23R, IL12A-AS1, TBL1XR1, FIP1L1, ADA, ABCC2, AK2, CCR1, CYBA, LYST, CFTR, DIS3L2, CD79B, CD79A, ALB, UNC13D, SLC19A3, ACAT1, ALPL, ABL1, CRP, PARP1, PCDH19, AMBP, HSPA1A, MAPK1, PAEP, HSPA1B, CSF2, SARDH, CASP1, NR1I2, SOD1, VEGFA, SRL, ABCB1, BAG3, AHSA1, HDGFL2, CEACAM5, POLDIP2, NFE2L2, RNF19A, GRAP2, HTRA3, AIMP2, COL11A2, MTCO2P12, LAMC2, CRK, MAPK14, ROS1, MPO, PDR, LINC01672, MBL2, CD274, IFNA13, UBE2B, UCP1, IL18, MMP9, MMP2, HSP90B2P, TRPV4, SMIM10L2B, GABPA, SLC17A5, AMCN, IFNA1, CASP9, APEX1, SMIM10L2A, SMARCB1, HSPD1, SERPINE1, TRPA1, CS, BRAF, BECN1, MRC1, TBC1D9, BAX, TNFSF10, ACTB, SCN5A, PKD2L1, COX8A, MAPK8, CCHCR1, CD163, VWF, CHRM3, ARIH1, MTX1, MYB, DDX53, ANXA5, TGFB1, TLR2, MB, GAPDH, LEP, BATF2, NR3C1, DECR1, ERN1, ACE, LCN2, FLT4, IGF1, NR5A1, HSPA5, F2, GPI, EPHB2, HIF1A, EMP1, DNM1L, IL17A, ILK, P2RX7, AKT1, APOE, OGG1, NDRG2, CENPV, INSRR, NPS, NTS, MAP2K7, RAD51, IRF1, ABCG2, RECQL4, ESR1, MAVS, ICAM1, NOX3, IL13, ARSD, PLK1, IL37, PLAT, ERBB2, CD19, UBXN11, FHL3, TIMP1, IGFBP6, ANGPT2, EGFR, ELN, IGFALS, ATF6, IFNB1, IL4, PHB2, TSL, PRDX2, PTGS1, ARSA, EIF2AK1, ADGRV1, DCTN6, TSPO, FCGR1A, LBP, DBP, DNAJB1P1, MSH3, ELP1, ABCC1, MRE11, SOCS3, FUT1, SELENBP1, DNAJB1, NBAS, BDNF, GCHFR, TNFRSF11A, TLR9, SHBG, MECP2, MDM4, HSPA7, CCL2, LYZ, CCL3, HSPA6, PERCC1, IL2RA, DIO2, NQO1, LOC102723971, CDR3, CIRBP, RSAD2, BRS3, ENOSF1, CXCR4, ITPA, S100A4, SNCA, LALBA, COG6, CRLF1, ARHGAP24, MIR92B, GPHN, MT4, AKR1A1, KHDRBS1, IFITM2, ABCC4, PDLIM5, KAT8, ALS2, MIR377, IFITM3, DDX17, SNORD116@, SEMA6A, CDNF, MIR34A, STUB1, FAM107B, APBB3, ZNRD2, SYTL1, GRIN3A, MSLN, GPR50, HDAC11, PPR1, ERVW-4, PGR-AS1, GORASP1, SLC22A8, LONP1, ACBD3, PPIG, LOC102724197, EXO5, IL25, LINC02210-CRHR1, MTA1, TMC7, UPK3B, CCRL2, MARCKSL1, MSPC, WNK1, FRTS1, FTO, EIF2S2, ERVK-32, CARD14, NOX5, H3P23, SQSTM1, OTOF, STOML1, DHRS2, MVP, TSHZ1, MIR190B, MED25, GBA3, IL18BP, ABCB6, AD14, TMED7-TICAM2, POLD4, MAP1LC3B, SRA1, HAMP, FAS-AS1, WDR1, FBRS, RGP1, NFAT5, GRHL3, MTRNR2L13, ISG15, CLOCK, APOBEC3G, ERVK-6, H6PD, WLS, KIF23, IFIH1, EIF2AK3, HDAC9, RGPD1, NES, B3GAT1, GPBAR1, ATF7IP, HSPA14, DCTN4, SLC2A12, TRNT1, TRPV3, RNF114, ZC4H2, TMED7, PER2, NOX4, DUOX2, MYDGF, SLC2A8, CLYBL, APOBEC3A, STX1B, TBK1, SETD2, REM1, SAT2, SGSM3, APOBEC3C, SESN1, GPKOW, GLS2, CDCA5, DNAJA4, SLC46A1, HIKESHI, FEV, TWIST2, AHI1, DYM, KRT20, C14orf28, STX18, SOCS4, RBM45, CGAS, SARS2, IL23A, ISYNA1, TICAM1, AHSA2P, MOCOS, XKR8, PRRX2, SUCO, NIP7, PDCL2, SLCO6A1, DUSP13, FBXW7, TRIM69, CDAN1, CACYBP, COPD, LILRB1, POLE4, TICAM2, GSTK1, DOLK, TDGF1P6, FAM89A, MALAT1, ARMS2, STK38, GDF6, FBLIM1, TREH, MIR142, PSIP1, CD160, MIR143, SDS, SLC25A21, CLP1, MIR21, IFI44L, PRDX3, GADD45G, MIR22, PPARGC1A, MIR23A, MIR27B, GALP, DICER1, SIRT1, SLC35B2, GJD2, SIGLEC7, NOX1, DNAI1, IFNL3, MUC16, SMR3A, IFNL1, FGF21, FBXO8, BLOC1S2, GOPC, DNER, OR10A4, TSPAN33, SETBP1, GGTLC1, AICDA, TFIP11, HSPBP1, NUP62, DAPK2, CYP20A1, PES1, ISCU, MLYCD, NLRP12, HPGDS, PROX1, CDK5R1, FGFR1, FLT1, FN1, FOLH1, FXN, MTOR, FSHMD1A, GABRA2, GC, GCG, GCH1, GFAP, GH1, GJA1, GLB1, GLI2, GLP1R, GNAS, FLNA, FGF14, DCX, FGF7, DPP4, ATN1, DUT, E2F1, EGR1, ELK3, EPHB1, EREG, EXT1, EXTL3, F8, F13A1, FANCD2, PTK2B, FCN2, FDXR, FGF4, GNRH1, GNRH2, GPX1, GRM1, IL12RB1, CXCL10, IRF3, IRF5, ISG20, ITGAM, ITGB2, ITGB3, KCNC1, KCNQ2, KDR, KNG1, KRAS, RPSA, LEPR, LGALS1, LHX1, CXCR2, IL6ST, IL5, HFE, GRM2, CXCL1, CXCL3, GRPR, GSTT1, GTF2H1, HCLS1, HLA-A, IL2RB, HP, AGFG1, HSPA8, HTR5A, ICAM2, IFI27, CCN1, DEFB1, CD55, PROM1, APOB, AQP5, ARRB1, STS, ARSF, ASL, B2M, BAAT, HCN2, CEACAM1, FOXL2, BPI, BRCA1, C4BPA, VPS51, CA9, CAD, CALB1, FASLG, APOA1, CYP3A5, ANXA1, NAT2, ACHE, ADAR, ADCYAP1, ADH1A, ADH1B, ADH1C, ADH4, AGER, JAG1, AGT, AGTR2, AIF1, AKT2, AKR1B1, ALS3, ANPEP, CALCR, CAMLG, CANX, CASP6, CISH, CNA1, COL12A1, SLC31A1, CPT1B, CRHR1, CRMP1, CRYZ, CSN2, CSN3, CSNK2B, VCAN, CST3, CSTB, CTNNB1, CTSL, CUX1, CHKB, CHKA, CEACAM7, TNFRSF8, CASP8, CASQ1, SERPINA6, CD2, CD9, CD14, MS4A1, CD34, CEACAM3, CD38, CD40, CD44, CD58, CD59, CDC42, CDKN2A, LMNB1, CD180, EPCAM, SLA, SLC6A2, SLC6A3, SLC19A1, SLCO2A1, SNAP25, SOAT1, SOX10, SRF, SSTR1, STAT1, STAT5A, SYT1, ADAM17, TAT, TCOF1, TERT, TGFB2, SLC6A1, ST3GAL4, MAA, SRSF1, RAC1, RBM3, RDX, RELA, REN, ROM1, RRAD, S100A1, S100B, SAI1, SARS1, ATXN1, SCN2A, CX3CL1, CXCL12, SEA, SELPLG, TGFB3, THBS1, TLR3, TLR5, SLMAP, NR4A3, SHOC2, FGF23, MIA, PLA2G6, KLF11, DENR, KHSRP, TNFSF11, DYNLL1, TNFRSF25, RAB11A, SUCLA2, CES2, SOCS2, HDAC3, XRCC5, XK, XBP1, TUB, TNFRSF1B, TP53BP1, TP73, TRAF6, TRE-TTC3-1, TRH, TRPM2, TTR, VEGFC, TWIST1, TYMS, UCP3, UMOD, NR1H2, UTRN, VCAM1, RAB5A, PVR, PTX3, SERPINA5, MX1, NEDD9, NFKB1, NHS, NM, NOS2, NPY, NPPA, NPPB, NTSR1, OAS2, OAS3, ODC1, OLR1, OTC, PAM, REG3A, MUC2, MUC1, MTHFR, CD99, MAPT, MAS1, MATK, MAX, SMCP, MEOX2, KITLG, MLH1, MTAP, MMP10, MMP14, MNAT1, CD200, MSD, MSH2, MSR1, PC, PCK1, PTPN11, PCNA, PPP3R1, PRKCA, PRKCD, PRKDC, MAPK7, PROP1, NAT1, PSEN1, PSG2, PSG5, PSMA7, PSMB8, PSMD1, PSMD4, PSMD9, PTEN, PTGER3, PPOX, PPARA, PPA1, PIK3CB, PDB1, PDCD1, PDK1, PEPC, PEX13, PF4, PIK3CA, PIM1, POU2F2, PIK3CD, PIK3CG, PI4KB, PLA2G1B, PLA2G2A, PLG, POU2F1, H3P5
-
Corneal Neovascularization
Wikipedia
For contact lenses related hypoxia , ceasing the use of contact lenses is the first step until corneal neovascularization is addressed by a physician. ... Topical administration of steroids and non-steroid anti-inflammatory drugs are first-line treatment for individuals with CNV.VEGFA, FGF2, FLT1, MUC4, ITGAV, CYP1B1, GP1BB, GJB2, FOXE3, TBX1, JMJD1C, NLRP1, GJB6, NGLY1, SEC24C, COMT, ARVCF, UFD1, HIRA, RREB1, MMP9, COL18A1, KDR, PECAM1, IL1B, PROX1, CCL2, HIF1A, PLG, TAC1, NTN4, MIR1246, MIR132, CTNNB1, MIR184, ADAMTS9, MXRA7, WNT1, VIM, MIR223, VEGFC, MIR296, TLR4, MIAT, CXCR4, C20orf181, TLR3, MIR1275, TIMP1, TEK, MIR211, BCL10, RIPK1, SLURP1, MIR206, ANGPTL1, ADIPOQ, NTN1, PCLAF, MIR204, MIR155, LYVE1, CD160, TRAM1, TICAM2, IL1F10, ANGPT4, TMED7, AAVS1, TACR1, SEMA3F, HGF, CXCL1, GLI3, GLB1, FOXC2, FGF7, EMP2, EGF, EDNRB, ECM1, DMD, DCN, CHRM3, VPS51, TSPO, CEACAM1, ARF1, APOE, ANGPT2, ALB, AKT1, ICAM1, IKBKB, IL1RN, MMP14, CXCL12, PTAFR, PPARA, PLXNA2, AGT, PLAT, SERPINF1, PDGFRB, NRF1, MMP13, IL6, MMP12, MMP3, MMP2, LGALS3, KRT13, KRT3, IRS1, INSR, CXCL8, TMED7-TICAM2

- Neurosis Wikipedia
-
Kashin–beck Disease
Wikipedia
To date, more than a million individuals have suffered from KBD. [2] The symptoms of KBD include joint pain, morning stiffness in the joints, disturbances of flexion and extension in the elbows, enlarged inter-phalangeal joints, and limited motion in many joints of the body. [3] Death of cartilage cells in the growth plate and articular surface is the basic pathologic feature; this can result in growth retardation and secondary osteoarthrosis . [1] Histological diagnosis of KBD is particularly difficult; clinical and radiological examinations have proved to be the best means for identifying KBD. [4] Little is known about the early stages of KBD before the visible appearance of the disease becomes evident in the destruction of the joints. [4] This disease has been recognized for over 150 years but its cause has not yet been completely defined. [1] Currently, the accepted potential causes of KBD include mycotoxins present in grain , trace mineral deficiency in nutrition , and high levels of fulvic acid in drinking water . [1] Selenium and iodine have been considered the major deficiencies associated with KBD. [1] Mycotoxins produced by fungi can contaminate grain, which may cause KBD because mycotoxins cause the production of free radicals . [1] T-2 is the mycotoxin implicated with KBD, produced by members of several fungal genera. [5] T-2 toxin can cause lesions in hematopoietic , lymphoid , gastrointestinal , and cartilage tissues, especially in physeal cartilage. [5] Fulvic acid present in drinking water damages cartilage cells. [1] Selenium supplementation in selenium deficient areas has been shown to prevent this disease. [1] However, selenium supplementation in some areas showed no significant effect, meaning that deficiency of selenium may not be the dominant cause in KBD. [1] Recently a significant association between SNP rs6910140 of COL9A1 and Kashin–Beck disease was discovered genetically, suggesting a role of COL9A1 in the development of Kashin–Beck disease. [6] Contents 1 Cause 2 Prevention 3 Treatment 4 Epidemiology 5 Eponymy 6 See also 7 References 8 External links Cause [ edit ] The cause of KBD remains controversial.ITPR2, TXNRD2, HLA-DRB1, DIO2, ACAN, CHST13, PIK3CG, PIK3CD, PIK3CB, PIK3CA, GPX1, IL1A, FRZB, IL1B, IL6, CTNNB1, GDF5, VEGFA, FAS, CHST12, CASP3, TNF, GPX4, ADAM12, FZD1, TGFBR1, FADD, ADAMTS1, SELENOF, ADAMTS4, PPARGC1B, SFXN1, HS6ST2, ATG4C, ZGPAT, SELENOS, ASPN, CHST11, ABI3BP, CD2AP, MPRIP, ADAMTS5, RIPK3, UST, TACR1, TGFB1, NFE2L2, SELENOP, RAN, BAX, BCL2, BGN, C5, CASP8, COL2A1, COL9A1, COL10A1, COL11A1, HAPLN1, DAPK3, DCN, CFD, FGF8, FGF12, FGFR3, GABPA, GPR18, GPX3, HABP2, IGFBP2, IGFBP3, CD46, MMP1, MYC, PTHLH, RAC2, MIR23B

-
Dysplastic Nevus
Wikipedia
A small percent of these individuals are members of melanoma kindreds. [12] Inherited dysplastic nevus syndrome is an autosomal dominant hereditary condition. Dysplastic nevi are more likely to undergo malignant transformation when they occur among members of melanoma families.CDK4, CDKN2A, BRAF, NRAS, H3P10, CCND1, MC1R, TP53, CTSD, MIR211, CD82, CDK6, GSTT1, CXCL1, XRCC1, STAT3, TCHH, KAT5, RECQL4, TRH, TNF, BCL2, TGFA, TERT, PRAME, TERF2, SSX2, SOX4, FSCN1, SMARCB1, PMEL, SCN8A, S100A8, U2AF2, LRIT1, AMACR, SESN2, SSX2B, MIR21, MIR144, MIR106B, MIRLET7B, MIA3, KRT25, TNS4, RNASE7, SHCBP1, CADM1, FBXW7, ING3, RTEL1, ING4, IL22, GNMT, BBC3, RHCE, BRMS1, S100A7, CLDN11, MAPK1, HLA-B, GSTM1, GHRH, ETS1, EPHB2, EIF4E, EGFR, EDNRB, DUSP3, DRG2, CSF2, COMP, COL9A3, COL9A2, COL9A1, CMM, AR, ARNT, CD1C, CCND3, HCL2, HNRNPK, PIN1, IGFBP7, PAM, BRCA1, OSM, AQP1, NME1, MSH2, MRC1, MMP13, MMP2, MMP1, MLH1, MIF, MDM2, LGALS3, LGALS1, LAMC2, IL18, IL13, IL1B, APOE

-
Optic Disc Drusen
Wikipedia
About two thirds to three quarters of clinical cases are bilateral. [1] A necropsy study of 737 cases showed a 2.4% incidence with 2 out of 15 (13%) bilateral, [2] perhaps indicating the insidious nature of many cases. An autosomal dominant inheritance pattern with incomplete penetrance and associated inherited dysplasia of the optic disc and its blood supply is suspected. [20] [21] Males and females are affected at equal rates.

-
Genu Valgum
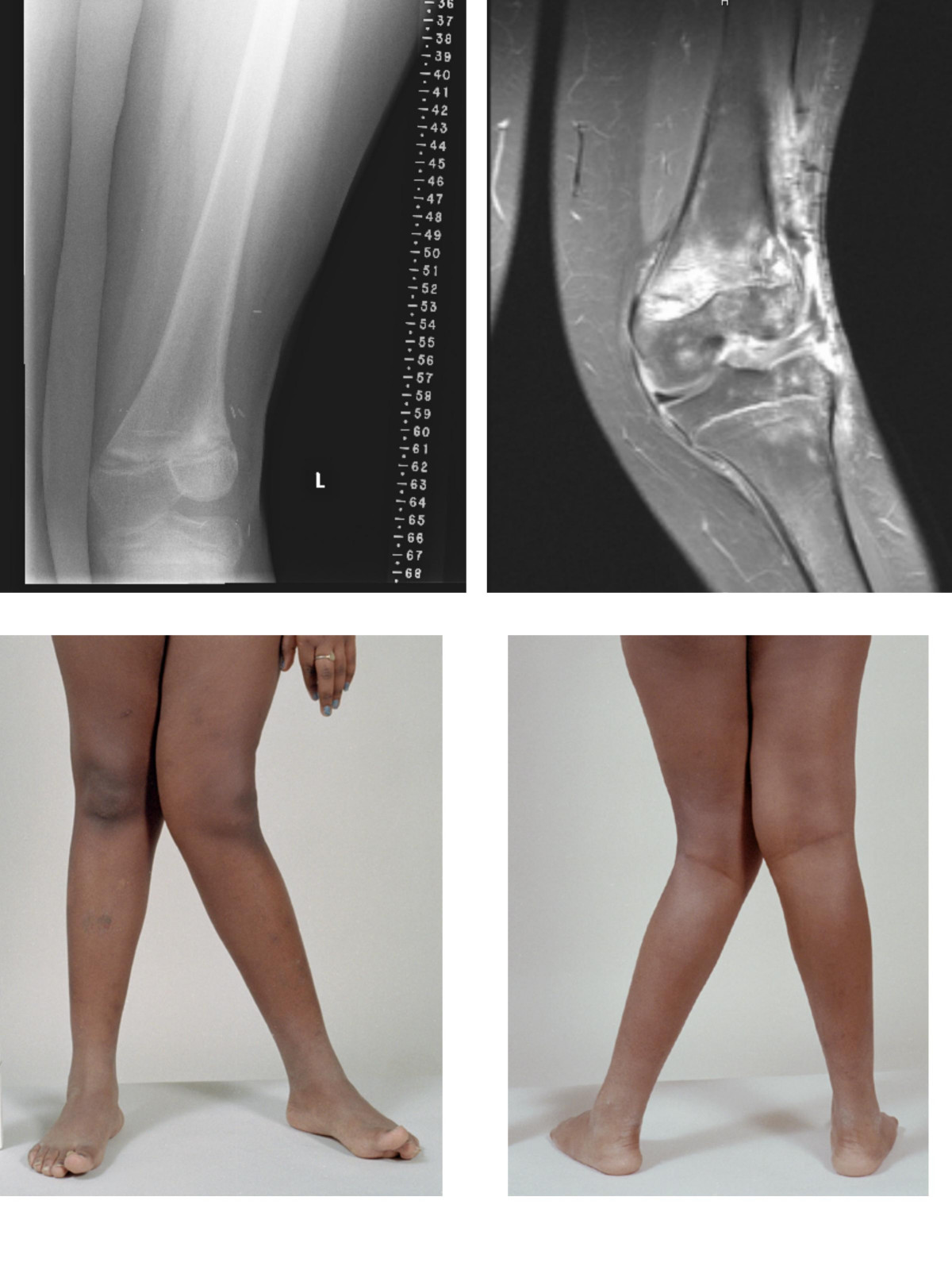
Wikipedia
Other systemic conditions may be associated, such as Schnyder crystalline corneal dystrophy , an autosomal dominant condition frequently reported with hyperlipidemia .ACTA1, HERC2, NPAP1, SPART, COG5, TUBB3, KLHL41, APC2, MKRN3-AS1, GTF2IRD1, CHST3, EIF2AK3, LONP1, BAZ1B, SYNGAP1, PTCH1, TNFSF11, GAN, MKRN3, CLIP2, VDR, TRPS1, TPM2, TGFB1, SNRPN, SKI, SHOX, SFRP4, AUTS2, ZBTB20, TBL2, SETD2, PWRN1, KIF7, SNORD115-1, VPS13B, PWAR1, EVC2, B3GALT6, LOXL3, GNPTG, SLC10A7, RAB33B, CTC1, NSD1, IFIH1, TRPV4, LMOD3, MCTP2, IARS2, IFT57, IMPAD1, BCOR, DYM, MAGEL2, RAB23, DYNC2LI1, RFC2, MAP2K2, ACAN, COL9A2, EXT2, EXT1, EVC, ELN, MEGF8, SLC26A2, CYP19A1, CTNS, CPT2, COMP, COL11A1, COL9A3, COL9A1, MAP2K1, COL2A1, CLCN7, CFL2, CBS, SERPINH1, RUNX2, CA2, BRAF, NKX3-2, ATRX, ATP7A, ARSB, FBN1, FLNA, FN1, GALNS, PEPD, ENPP1, ORC1, OCRL, NOTCH2, TONSL, NF1, NEB, NDN, MMP13, MATN3, LIMK1, LIFR, KRAS, KIF22, IPW, IDUA, HSPG2, HBB, GUSB, GTF2I, GLI1, GLB1, SNORD116-1, IL2RG, GHRHR
-
Glycogen Storage Disease Ixb
OMIM
Burwinkel et al. (1997) reported 3 children, including 2 sibs, with GSD IXb. The first child was German, and presented at age 22 months with distended abdomen due to hepatomegaly.
- Chronic Granulomatous Disease MedlinePlus
-
Amyotrophic Lateral Sclerosis 5, Juvenile
OMIM
INHERITANCE - Autosomal recessive HEAD & NECK Face - Increased facial reflexes - Jaw spasticity - Weak masseter muscles Mouth - Tongue weakness - Poor palatal elevation RESPIRATORY - Respiratory failure due to muscle weakness MUSCLE, SOFT TISSUES - Distal muscle weakness - Distal muscle atrophy - Chronic neurogenic changes seen on EMG - Fibrillations - Fasciculations NEUROLOGIC Central Nervous System - Upper motor neuron signs - Lower motor neuron signs - Pyramidal signs - Spasticity - Hyperreflexia - Extensor plantar responses - Bulbar signs - Dysarthria - No cognitive impairment - No thinning of corpus callosum - Loss of anterior horn cells in the spinal cord - Loss of myelinated fibers in the anterolateral columns Peripheral Nervous System - Decreased amplitude of compound muscle action potentials MISCELLANEOUS - Onset in first or second decade - Slowly progressive - Some patients may become wheelchair-bound - Survival 30 to 40 years after onset MOLECULAR BASIS - Caused by mutation in the spatacsin gene (SPG11, 610844.0003 ) ▲ Close
-
Type 1 Diabetes
MedlinePlus
Type 1 diabetes can occur at any age, from early childhood to late adulthood. The first signs and symptoms of the disorder are caused by high blood sugar and may include frequent urination (polyuria), excessive thirst (polydipsia), fatigue, blurred vision, tingling or loss of feeling in the hands and feet, and weight loss.
-
Dyshidrosis
Mayo Clinic
What to expect from your doctor Your doctor is likely to ask you questions, such as: When did you first notice your symptoms? Are your symptoms present all the time or only once in a while?

-
Carcinosarcoma
Wikipedia
Specialty Oncology Carcinosarcomas are malignant tumors that consist of a mixture of carcinoma (or epithelial cancer) and sarcoma (or mesenchymal / connective tissue cancer). [1] Carcinosarcomas are rare tumors, and can arise in diverse organs, such as the skin , salivary glands , lungs , the esophagus , pancreas , colon , uterus and ovaries . [1] [2] [3] [4] [5] [6] [7] Contents 1 Cellular origins 2 See also 3 References 4 External links Cellular origins [ edit ] Four main hypotheses have been proposed for the cellular origins of carcinosarcoma, based largely on the pathology of the disease. [1] [3] First, the collision tumor hypothesis, which proposes the collision of two independent tumors resulting in a single neoplasm , based on the observation that skin cancers and superficial malignant fibrous histiocytomas are commonly seen in patients with sun-damaged skin; second, the composition hypothesis, which suggests that the mesenchymal component represents a pseudosarcomatous reaction to the epithelial malignancy; third, the combination hypothesis, which suggests that both the epithelial and mesenchymal components of the tumor arise from a common pluripotential stem cell that undergoes divergent differentiation; and fourth, the conversion/divergence hypothesis, which argues that the sarcomatous component of the tumor represents a metaplastic sarcomatous transformation of the epithelial component.VIM, TGFB1, ZNF667-AS1, ERBB2, TP53, BRCA1, CDKN2A, H3P10, PIK3CA, BRAF, CD274, KRAS, KIT, EGFR, HMGA2, SYP, ZEB1, HTC2, ALK, MME, PDGFRA, MDM2, PTEN, PPP2R1A, DICER1, CLDN4, DCTN3, TGFBR1, LOC110806263, MIR200C, MIR184, S100A1, S100B, MIRLET7B, SMARCB1, SOX9, DCDC2, WT1-AS, NOX4, TOP1, HPS5, RACGAP1, CADM1, VEGFA, SMUG1, XRCC2, SATB2, PAX8, PHB2, CHP1, IFITM1, PTCH1, EMG1, TSHZ1, ACTB, PTPA, CLDN3, F2R, ESR1, EGF, ATN1, DYNC1H1, CTNNB1, CTAG1B, CDK4, FGFR2, VPS51, BRCA2, BCL2, CCND1, AR, ANGPT2, ANG, FBN1, GATA3, PPP1R1A, MLH1, PDCD1, PCNA, NME1, NCAM1, MYOG, MSH2, MMP2, MKI67, HMGA1, MET, MAGEA4, EPCAM, TACSTD2, IGF2, IGF1, FOXA2, NRAS










