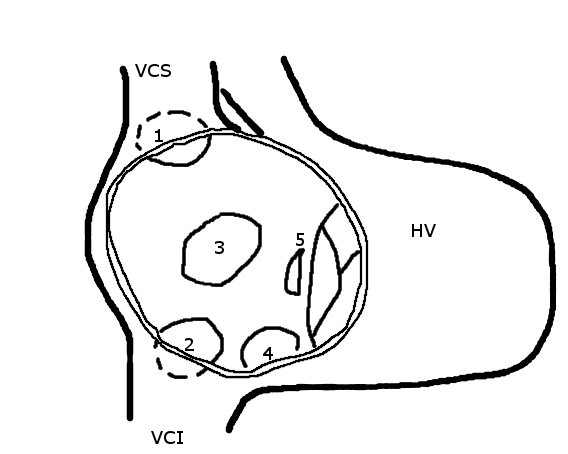
Branchial arch fistula Other names Benign cervical lymphoepithelial cyst Pharyngeal arch cyst Fistulogram (sinogram) of a right branchial cleft sinus. Specialty Medical genetics Symptoms Painless, firm mass lateral to midline, usually anterior to the SCM , which does not move with swallowing Causes Family history Differential diagnosis Vascular anomaly , dermoid cyst , thymic cyst , lymphadenopathy , lymphoma , HPV-related oropharyngeal cancer Treatment Conservative, surgical excision A branchial cleft cyst is a cyst as a swelling in the upper part of neck anterior to sternocleidomastoid . ... Persistence or abnormal formation of these four clefts can all result in branchial cleft cysts which may or may not drain via sinus tracts. First branchial cleft cysts account for 8% of the sinuses and cysts of the neck. ... Infection of the cysts in this region can compress trachea , causing respiratory problems, or it can compress the oesophagus , causing dysphagia , and irritating the sternocleidomastoid muscle, causing torticollis . [9] Third and fourth branchial cleft cysts are rare, usually consisting of 2% of all branchial arch abnormalities, located below the second branchial arch. They usually have sinus tracts that start from the anterior neck at the thyroid gland until pyriform sinus posteriorly. ... External links [ edit ] Pictures and Imaging of Branchial Cleft Cysts Classification D ICD - 10 : Q18.0 ( ILDS Q18.020) OMIM : 113600 MeSH : D001935 DiseasesDB : 1588 External resources MedlinePlus : 001396 eMedicine : derm/61 radio/107 v t e Congenital malformations and deformations of face and neck Face jaw : Otocephaly mouth : Macrostomia Microstomia lip : Macrocheilia Microcheilia chin : Microgenia multiple/other: Hallermann–Streiff syndrome Branchial cleft cyst Neck Webbed neck Ungrouped Preauricular sinus and cyst
A rare otorhinolaryngological malformation characterized by the presence of a cyst, sinus or fistula occuring along the anterior border of the sternocleidomastoid muscle.
Clinical Features The abnormality may be in the form of cysts, sinuses, or fistulas, the last term being reserved for those instances in which there is communication between the skin and the pharynx. These are considered to be anomalies of the second branchial cleft. Ear pits were also present in at least 1 family. Wheeler et al. (1958) found branchial cysts and sinuses in 4 members of 3 generations of a family. Cysts, sinuses, and skin tags containing cartilage occurred in a line extending from a point anterior to the ear to the anterior border of the sternomastoid muscle at the level of the angle of the mandible and thence along the anterior border of this muscle to a point near its attachment to the sternum. One must exclude the branchiootorenal (BOR) syndrome (113650) and the branchiootic (BO) syndrome (602588).
Makita et al. (2005) studied a Japanese boy who at 3 years of age presented with severe bradycardia and was diagnosed with sick sinus syndrome (see SSS1, 608567) with paroxysmal atrial fibrillation based on Holter ECG recordings. ... In a Japanese family in which an 11-year-old boy had sick sinus syndrome that progressed to atrial standstill, Makita et al. (2005) analyzed 3 cardiac ion channel genes previously associated with atrial standstill, atrial fibrillation, or sick sinus syndrome: SCN5A, HCN4 (605206), and GJA5. ... The proband's asymptomatic father had normal sinus rhythm with nonspecific ST depression in the inferior leads on ECG, whereas his unaffected mother and maternal grandmother had normal ECGs.
A number sign (#) is used with this entry because of evidence that atrial standstill-2 (ATRST2) is caused by homozygous mutation in the NPPA (108780) gene on chromosome 1p36. For a discussion of genetic heterogeneity of atrial standstill (AS), see ATRST1 (108770). Description Atrial standstill (AS) is a rare condition characterized by the absence of electrical and mechanical activity in the atria. On surface ECG, AS is distinguished by bradycardia, junctional (usually narrow complex) escape rhythm, and absence of the P wave. Nearly 50% of patients with AS experience syncope. AS can be persistent or transient, and diffuse or partial (summary by Fazelifar et al., 2005).
Contents 1 Characteristics 2 Diagnosis 3 Treatment 4 Prognosis 5 Epidemiology 6 See also 7 References Characteristics [ edit ] The most common sign of a nasal cyst is facial swelling, with obstruction of the nasal passage. [3] Sometimes, a mucoid nasal discharge occurs, which is caused by obstruction to mucociliary clearance , [3] and therefore does not resolve following antibiotic treatment. [4] If the cyst is located in the caudal maxillary sinus, it may cause the eyeball on the affected side to bulge out of the orbit, known as exophthalmos . [5] Diagnosis [ edit ] Radiographs generally provide better results than endoscopic examination when diagnosing these problems; multiloculated densities and fluid lines show up more readily in the sinuses, occasionally with dental displacement and also dental and jaw line distortion, flattened roots in the teeth, mineralization and soft tissue calcification, and major deviation of the septum and vomer bones. [ citation needed ] Treatment [ edit ] Cysts are removed by surgery, which may be performed with the horse standing and sedated, or under general anesthesia. [3] Treatment involves surgical removal of the cyst and any of the involved lining of the concha. Prognosis [ edit ] The prognosis for a complete recovery is good, and the rate of any recurrence is minimal. [5] Some horses may have a mild mucous discharge after surgery, which can be permanent. [1] Epidemiology [ edit ] Most nasal cysts are identified in horses younger than one year old, but can also be diagnosed in horses over 9 years of age. [1] There is no known breed or sex predisposition for nasal cysts. [4] See also [ edit ] Ethmoid hematoma References [ edit ] ^ a b c Rush, Bonnie R. (2019). "Sinus cysts" . The Merck Veterinary Manual . Retrieved 2019-10-26 . ^ Rush, Bonnie; Mair, Tim (2008). "Paranasal sinus cysts". Equine Respiratory Diseases .
Often, craniofacial osteoma presents itself through ocular signs and symptoms (such as proptosis ). [1] Contents 1 Variants 2 See also 3 References 4 External links Variants [ edit ] " Osteoma cutis , but there is currently no way of detecting if and when this is likely to occur. " Fibro-osteoma " " Chondro-osteoma " Osteoma of the frontal sinus seen on x-ray Osteoma of the frontal sinus on CT Osteoma See also [ edit ] Osteosclerosis Familial adenomatous polyposis Exostosis Gardner syndrome Ganglion cyst References [ edit ] ^ Michael S. ... "Management of a Large Frontoethmoid Osteoma with Sinus Cranialization and Cranial Bone Graft Reconstruction" .
A crooked septum — the wall between the nostrils — may restrict or block sinus passages, making the symptoms of sinusitis worse. ... Infections in your respiratory tract — most commonly colds — can inflame and thicken your sinus membranes and block mucus drainage. ... A skin test is safe and quick and can help detect what allergen is responsible for your nasal flare-ups. Samples from your nasal and sinus discharge (cultures). Cultures are generally unnecessary for diagnosing chronic sinusitis. ... Surgery In cases resistant to treatment or medication, endoscopic sinus surgery might be an option. For this procedure, the doctor uses a thin, flexible tube with an attached light (endoscope) to explore your sinus passages. Depending on the source of the blockage, the doctor might use various instruments to remove tissue or shave away a polyp that's causing nasal blockage. Enlarging a narrow sinus opening also may be an option to promote drainage.
Heart rate that exceeds the normal resting rate Tachycardia Other names Tachyarrhythmia ECG showing sinus tachycardia with a rate of about 100 beats per minute Pronunciation Tachycardia / t æ k i ˈ k ɑːr d i ə / , tachyarrhythmia / t æ k i ə ˈ r ɪ ð m i ə / Specialty Cardiology Differential diagnosis Palpitations , Ventricular tachycardia , Supraventricular tachycardia , Paroxysmal tachycardia , Junctional ectopic tachycardia , Sinus tachycardia , Atrial tachycardia , AV nodal reentrant tachycardia Tachycardia , also called tachyarrhythmia , is a heart rate that exceeds the normal resting rate . [1] In general, a resting heart rate over 100 beats per minute is accepted as tachycardia in adults. [1] Heart rates above the resting rate may be normal (such as with exercise ) or abnormal (such as with electrical problems within the heart). Contents 1 Complications 2 Causes 3 Diagnosis 3.1 Differential diagnosis 3.1.1 Sinus 3.1.2 Ventricular 3.1.3 Supraventricular 3.1.3.1 Atrial fibrillation 3.1.3.2 AV nodal reentrant tachycardia 3.1.3.3 AV reentrant tachycardia 3.1.3.4 Junctional tachycardia 4 Management 4.1 Unstable 5 Terminology 6 See also 7 References 8 External links Sound of a student's heart during tachycardia. ... Causes [ edit ] Some causes of tachycardia include: Adrenergic storm Anaemia Anxiety Atrial fibrillation Atrial flutter Atrial tachycardia AV nodal reentrant tachycardia Brugada syndrome Early manifestation of circulatory shock Dysautonomia Exercise Fear Hypoglycemia Hypovolemia Hyperthyroidism Hyperventilation Junctional tachycardia Multifocal atrial tachycardia Pacemaker mediated Pain Pheochromocytoma Sinus tachycardia Sleep deprivation [4] Supraventricular tachycardia Ventricular tachycardia Wolff–Parkinson–White syndrome Drug related: Alcohol Stimulants Cannabis (drug) Drug withdrawal Tricyclic antidepressants Nefopam Opioids (rare) Diagnosis [ edit ] The upper threshold of a normal human resting heart rate is based on age. ... Tachycardias can be further classified as either regular or irregular. Sinus [ edit ] Main article: Sinus tachycardia The body has several feedback mechanisms to maintain adequate blood flow and blood pressure . ... Hyperthyroidism can also cause tachycardia. [9] The upper limit of normal rate for sinus tachycardia is thought to be 220 bpm minus age.
Types There are many different types of tachycardia. Sinus tachycardia refers to a typical increase in the heart rate often caused by exercise or stress. ... It can be a usual rise in heart rate caused by exercise or a stress response (sinus tachycardia). Sinus tachycardia is considered a symptom, not a disease. ... The heart's rhythm is controlled by a natural pacemaker (the sinus node) in the right upper chamber (atrium). The sinus node sends electrical signals that normally start each heartbeat. ... Less commonly, it may be used to evaluate sinus tachycardia. In this test, a health care provider threads thin, flexible tubes (catheters) tipped with electrodes through the blood vessels to different areas within the heart.
Odontogenic sinusitis is an inflammatory condition of the paranasal sinuses that is the result of dental pathology, most often resulting from prior dentoalveolar procedures, infections of maxillary dentition, or maxillary dental trauma. [5] Infections associated with teeth may be responsible for approximately 20% of cases of maxillary sinusitis. [6] The cause of this situation is usually a periapical or periodontal infection of a maxillary posterior tooth, where the inflammatory exudate has eroded through the bone superiorly to drain into the maxillary sinus . Medical management and treatment of the underlying dental pathology remains a critical initial step in the treatment of odontogenic sinusitis, however recent literature suggests that a significant portion of patients may require endoscopic sinus surgery for successful disease resolution. [5] Once an odontogenic infection involves the maxillary sinus, it is possible that it may then spread to the orbit or to the ethmoid sinus . [6] CT showing complete opacification of the right maxillary and right anterior ethmoid sinuses with associated involvement of the ostiomeatal unit.
The cause of the arrhythmia, the ectopic focus, is usually near the AV node in the triangle of Koch (a rough triangle with points at the coronary sinus, the tendon of Todaro, and the tricuspid valve). [4] Patients of heart surgery may experience an accelerated narrow complex tachycardia, usually within the first 24–48 hours (but occasionally longer) after surgery. ... In this case the right bundle branch block was present during tachycardia and during normal sinus rhythm. JET is most commonly diagnosed using a 12-lead ECG. ... External links [ edit ] Classification D MeSH : D013613 v t e Cardiovascular disease (heart) Ischaemic Coronary disease Coronary artery disease (CAD) Coronary artery aneurysm Spontaneous coronary artery dissection (SCAD) Coronary thrombosis Coronary vasospasm Myocardial bridge Active ischemia Angina pectoris Prinzmetal's angina Stable angina Acute coronary syndrome Myocardial infarction Unstable angina Sequelae hours Hibernating myocardium Myocardial stunning days Myocardial rupture weeks Aneurysm of heart / Ventricular aneurysm Dressler syndrome Layers Pericardium Pericarditis Acute Chronic / Constrictive Pericardial effusion Cardiac tamponade Hemopericardium Myocardium Myocarditis Chagas disease Cardiomyopathy Dilated Alcoholic Hypertrophic Tachycardia-induced Restrictive Loeffler endocarditis Cardiac amyloidosis Endocardial fibroelastosis Arrhythmogenic right ventricular dysplasia Endocardium / valves Endocarditis infective endocarditis Subacute bacterial endocarditis non-infective endocarditis Libman–Sacks endocarditis Nonbacterial thrombotic endocarditis Valves mitral regurgitation prolapse stenosis aortic stenosis insufficiency tricuspid stenosis insufficiency pulmonary stenosis insufficiency Conduction / arrhythmia Bradycardia Sinus bradycardia Sick sinus syndrome Heart block : Sinoatrial AV 1° 2° 3° Intraventricular Bundle branch block Right Left Left anterior fascicle Left posterior fascicle Bifascicular Trifascicular Adams–Stokes syndrome Tachycardia ( paroxysmal and sinus ) Supraventricular Atrial Multifocal Junctional AV nodal reentrant Junctional ectopic Ventricular Accelerated idioventricular rhythm Catecholaminergic polymorphic Torsades de pointes Premature contraction Atrial Junctional Ventricular Pre-excitation syndrome Lown–Ganong–Levine Wolff–Parkinson–White Flutter / fibrillation Atrial flutter Ventricular flutter Atrial fibrillation Familial Ventricular fibrillation Pacemaker Ectopic pacemaker / Ectopic beat Multifocal atrial tachycardia Pacemaker syndrome Parasystole Wandering atrial pacemaker Long QT syndrome Andersen–Tawil Jervell and Lange-Nielsen Romano–Ward Cardiac arrest Sudden cardiac death Asystole Pulseless electrical activity Sinoatrial arrest Other / ungrouped hexaxial reference system Right axis deviation Left axis deviation QT Short QT syndrome T T wave alternans ST Osborn wave ST elevation ST depression Strain pattern Cardiomegaly Ventricular hypertrophy Left Right / Cor pulmonale Atrial enlargement Left Right Athletic heart syndrome Other Cardiac fibrosis Heart failure Diastolic heart failure Cardiac asthma Rheumatic fever
Specialty Hematology Rosai–Dorfman disease , also known as sinus histiocytosis with massive lymphadenopathy or sometimes as Destombes–Rosai–Dorfman disease , [1] [2] [3] is a rare disorder of unknown cause that is characterized by abundant histiocytes in the lymph nodes or other locations throughout the body. [1] [4] Contents 1 Signs and symptoms 1.1 Lymphadenopathy 1.2 Extranodal disease 2 Cause 3 Diagnosis 3.1 Classification 4 Treatment 5 History 6 See also 7 References 8 External links Signs and symptoms [ edit ] The histiocytosis of Destombes–Rosai–Dorfman disease can occur in lymph nodes, causing lymphadenopathy , or can occur outside lymph nodes in extranodal disease. [ citation needed ] Lymphadenopathy [ edit ] Lymphadenopathy can occur in one or more groups of lymph nodes. ... PMID 16394460 . ^ a b c Foucar E, Rosai J, Dorfman R (1990). "Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): review of the entity". ... PMID 26966089 . ^ Sardana, D., Goyal, A. and Gauba, K., 2015. Sinus histiocytosis with massive lymphadenopathy: a “massive” misnomer. Diagnostic cytopathology, 43(4), pp.315-319. ^ Pulsoni A, Anghel G, Falcucci P, Matera R, Pescarmona E, Ribersani M, Villivà N, Mandelli F (2002). "Treatment of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): report of a case and literature review" . ... S2CID 25696348 . ^ Rosai J, Dorfman RF (1969). "Sinus histiocytosis with massive lymphadenopathy.
Rosai-Dorfman disease was first described by Rosai and Dorfman in 1969. It is a benign disease which is characterized by over-production and accumulation of a specific type of white blood cell ( histiocyte ) in the lymph nodes of the body, most often those of the neck (cervical). Other lymph node groups may also be involved and, in some cases, abnormal accumulation of histiocytes may occur in other areas of the body (extranodal). The cause of this condition remains unknown, although altered immune responses and infectious agents may play a role. Rosai-Dorfman disease is a self-limited and seldom life-threatening disease which commonly does not require therapy.
A rare non-Langerhans cell histiocytosis characterized by infiltration of lymph nodes or extranodal tissues by non-malignant histiocytes displaying emperipolesis, a non-destructive phagocytosis of lymphocytes or erythrocytes. Most typical presentation is as a massive cervical lymphadenopathy in adolescents and young adults. Most frequent sites of extranodal disease are skin, soft tissue, bones, paranasal sinuses, orbit, salivary glands, and central nervous system. Symptoms are related to mass effect in the affected organs.
A rare head and neck tumor characterized by a malignant epithelial neoplasm most commonly arising in the maxillary sinus or nasal cavity, occurring as a keratinizing, a non-keratinizing, or a spindle cell (sarcomatoid) type. Patients may present with nasal obstruction, epistaxis, rhinorrhea, swelling, or (at more advances stages) with facial pain and/or paralysis, diplopia, and proptosis. Patients with paranasal sinus tumors present later and at a higher stage than patients with nasal cavity carcinomas.
A rare head and neck tumor characterized by a malignant epithelial neoplasm with evidence of squamous differentiation, most commonly located in the piriform sinus, less frequently the posterior pharyngeal wall or the postcricoid area.
A rare head and neck tumor characterized by a firm infiltrative neoplasm with squamous differentiation, arising from the mucosal epithelium, and most commonly located in the tongue, floor of the mouth, or gingiva, but also the buccal mucosa or any other area of the oral cavity, depending on prevailing risk factors (such as smoking, alcohol consumption, and tobacco chewing). Patients present with a variably white, erythematous, mixed, nodular, or ulcerated lesion, which may cause discomfort, pain, or reduced mobility of the tongue. The tumor is aggressive with a propensity for local invasion and early lymph node metastasis.
Depending on the location, the cancer can cause abnormal patches or open sores (ulcers) in the mouth and throat, unusual bleeding or pain in the mouth, sinus congestion that does not clear, sore throat, earache, pain when swallowing or difficulty swallowing, a hoarse voice, difficulty breathing, or enlarged lymph nodes.
A rare head and neck tumor characterized by a malignant epithelial neoplasm with evidence of squamous differentiation, most commonly located in the supraglottis or glottis. The tumor can spread directly to adjacent structures or metastasize via lymphatic and blood vessels to regional lymph nodes, or lung, liver, and bones, respectively. Primary risk factors are tobacco smoking and (to a lesser extent) alcohol consumption. Patients may present with hoarseness, dyspnea, stridor, dysphagia, hemoptysis, or odynophagia.
A number sign (#) is used with this entry because of evidence that a mutation of the TNFRSF10B gene (603612.0001), alone or in combination with other genes, can cause squamous cell carcinoma of the head and neck. Mutations in the ING1 gene (601566) have been found in a small but significant number of cases of squamous cell carcinoma of the head and neck. Somatic mutation in the PTEN gene (601728) has also been found in cases of HNSCC. Pathogenesis The transforming growth factor beta family of 25-kD polypeptides (TGFB1, 190180; TGFB2, 190220; TGFB3, 190230) are potent inhibitors of epithelial cell growth. Acquisition of cellular resistance to growth inhibitors, such as TGFB1, may represent an important step in tumor development.
A rare head and neck tumor characterized by a malignant epithelial neoplasm with evidence of squamous differentiation, which may arise in association with high-risk HPV in a subset of cases. HPV-positive tumors have a strong predilection for the base of tongue and the palatine tonsils and typically present at an advanced clinical stage with cervical lymphadenopathy. They are associated with significantly better prognosis than HPV-negative tumors, which more commonly involve the soft palate, manifest as sore throat and difficulty in swallowing or a neck mass, and occur in older patients. Smoking and alcohol consumption are important risk factors.
A rare head and neck tumor characterized by a firm infiltrative neoplasm with squamous differentiation, most commonly arising at the vermilion border of the lower lip. Patients present with a usually asymptomatic lesion of variable appearance, such as ulceration, a focus of whitish thickening, a dry atrophic area, or an area of persistent chapping and localized flaking and crusting. Carcinomas of the lower lip tend to progress slowly (as opposed to those of the upper lip). Invasion of adjacent structures, including perineural spread, is typical, with a variable rate of metastasis, depending on the location.
In athletes, however, the resting heart rate can be as slow as 40 beats per minute, and be considered as normal. The term sinus arrhythmia [17] refers to a normal phenomenon of alternating mild acceleration and slowing of the heart rate that occurs with breathing in and out respectively. ... This can also be present during meditation breathing exercises that involve deep inhaling and breath holding patterns. [18] Bradycardias [ edit ] Normal sinus rhythm, with solid black arrows pointing to normal P waves representative of normal sinus node function, followed by a pause in sinus node activity (resulting in a transient loss of heart beats). ... This may be caused by a slowed signal from the sinus node (sinus bradycardia), by a pause in the normal activity of the sinus node (sinus arrest), or by blocking of the electrical impulse on its way from the atria to the ventricles (AV block or heart block). ... This is mediated by the sympathetic nervous system on the sinus node and called sinus tachycardia. ... Retrieved 13 April 2020 . ^ Hayano J (Feb 2004). "Respiratory sinus arrhythmia: why does the heartbeat synchronize with respiratory rhythm?".
This article needs additional citations for verification . Please help improve this article by adding citations to reliable sources . Unsourced material may be challenged and removed. Find sources: "Premature heart beat" – news · newspapers · books · scholar · JSTOR ( March 2015 ) ( Learn how and when to remove this template message ) Premature heart beat A premature ventricular contraction marked by the arrow. Specialty Cardiology A premature heart beat is a heart rhythm disorder corresponding to a premature contraction of one of the chambers of the heart. Premature heart beats come in two different types, premature atrial contractions and premature ventricular contractions . Often they cause no symptoms but may present with fluttering in the chest or a skipped beat.