-
Yellow Fever
Orphanet
Vaccination is contraindicated in children <4 months old and pregnant women and caution is advised in persons with egg allergy, the immunocompromised, children 4-9 months of age and elderly persons, especially if the risk is minimal, such as trips restricted to attending conferences in modern urban hotels with no rural exposure. Prognosis Case fatality rates in symptomatic cases are 20-50%.ERVK-32, ERVK-6, DDOST, PARTICL, TRIM56, CYP20A1, EMC3, TRAV12-2, BACE1, AMACR, TRPA1, TFPI, RPL19, RAF1, CRP, MRC1, IL10, IL6, IL1RN, IFNG, IFNAR1, GYPC, GPT, GLS, FCGR3B, FCGR3A, F10, MAP2K1

-
Pneumonoultramicroscopicsilicovolcanoconiosis
Wikipedia
The word featured in the headline for an article published by the New York Herald Tribune on February 23, 1935, titled "Puzzlers Open 103rd Session Here by Recognizing 45-Letter Word": Pneumonoultramicroscopicsilicovolcanoconiosis succeeded electrophotomicrographically as the longest word in the English language recognized by the National Puzzlers' League at the opening session of the organization's 103rd semi-annual meeting held yesterday at the Hotel New Yorker. The puzzlers explained that the forty-five-letter word is the synonym of a special form of pneumoconiosis caused by ultra-microscopic particles of silica volcanic dust ...
-
Legg-Calve-Perthes Disease
Mayo Clinic
To keep the ball part of the joint as round as possible, doctors use a variety of treatments that keep it snug in the socket portion of the joint. The socket acts as a mold for the fragmented femoral head as it heals. ... During healing, the socket part of the joint can serve as a mold to help the fragmented femoral head retain its round shape. For this molding to work, the femoral head must sit snugly within the socket.COL2A1, CREBBP, EP300, EXT1, TRPS1, INPP5K, NAGLU, UFSP2, ATP7A, TRPV4, FZD2, SIL1, WNT5A, ADAMTS2, DVL3, DVL1, GNPTAB, COMP, COL1A2, COL1A1, SLC2A10, F5, MIR214, SRCAP, MIR206, SERPINC1, NR4A3, TNF, SOX9, MTHFR, IL6, FGB, COX8A, BGLAP, BAX, LPA

-
Chagas Disease
Mayo Clinic
Triatomine bugs live primarily in mud, thatch or adobe huts in Mexico, South America and Central America. They hide in crevices in the walls or roof during the day and come out at night — often feeding on sleeping humans. ... You may also become infected by: Eating uncooked food contaminated with feces from bugs infected with the parasite Being born to a person who is infected with the parasite Getting a blood transfusion or an organ transplant from someone who was infected with the parasite Being accidentally exposed to the parasite while working in a lab Spending time in a forest that contains infected wild animals, such as raccoons and opossums Risk factors The following factors may increase your risk of getting Chagas disease: Living in poor rural areas of Central America, South America and Mexico Living in a residence that contains triatomine bugs Receiving a blood transfusion or organ transplant from a person who carries the infection It's rare for travelers to the at-risk areas in South America, Central America and Mexico to catch Chagas disease because travelers tend to stay in well-constructed buildings, such as hotels. Triatomine bugs are usually found in structures built with mud or adobe or thatch.CYP51A1, TNF, IL10, IFNG, MMP2, LGALS3, CCR5, PPARG, MMP9, IL2, HLA-A, HLA-DRB1, HSPA4, MTCO2P12, IL6, IL17A, MBL2, TLR4, COX2, IL18, IL1B, PTGS2, RBM45, CALR, PPP1R2C, TLR2, NFE2L2, NDUFA5, TGFB1, MYD88, CYTB, REN, IL1RN, NLRP3, ACHE, APOA1, ATM, PRL, VIP, TP53, VDR, KNG1, HP, TPI1, FN1, TLR9, CTSL, TRIM33, CYP2B6, ACE, BACE1, EPGN, NPNT, CCL4, CCL3, SPN, AMZ1, CCL2, THBS1, RRAD, TNFRSF1B, MIR208A, CCR2, SPINK1, CX3CL1, SDC4, SKIL, SLC11A1, SMPD1, SOD2, TRBV20OR9-2, KIR2DS2, TCN2, TWIST1, RO60, TRIM21, SRM, ROS1, COLEC11, PPARGC1B, PANX1, MASP2, PPARGC1A, SBNO2, SIRT2, RPIA, PLCB1, SIRT1, PTPN22, EBI3, PYCARD, HSPA14, UBAP1, GGNBP2, SBNO1, OTUB1, RABEP2, HEXIM1, KNTC1, TYK2, TNFSF11, VIM, VIPR1, VPS11, FOSL1, CDR3, DYSF, DBA2, TP63, ARHGEF10, MCU, ADAM7, EIF2S2, LMLN, MBD2, SLC25A31, TMPRSS11D, VIPR2, ABO, RAD51, CSF3, CYBB, DECR1, DHODH, DMD, EIF2S1, EIF2S3, FBN1, FCN2, FDPS, FHIT, FOXO3, GAST, G6PD, GABPA, GCK, GEM, GLUL, CTSB, CR1, HLA-G, CDKN1A, ACTB, ADA, PARP1, AGT, ALB, ALOX5, ARG1, STS, ATP2A3, ATP2B1, BCHE, BDNF, C3, CACNA1C, CAMP, CD80, CD86, HLA-DPB1, HSPD1, PPBP, COX1, NGF, NHS, NOS2, PNP, NRF1, OCA2, P2RX7, PAEP, PCNA, PDE2A, PIK3CA, PIK3CB, PIK3CD, PIK3CG, PLCB4, POLG, POMC, PPP1R12A, MIF, IGF1, MEF2D, IGHG3, IL2RA, IL4R, IL7, IL12B, IL13, IL15, ISG20, ITPR1, KIR2DL2, KIR3DL1, KRT8, LGALS9, LTA, LY6E, MAP6, MEF2A, NT5E

-
Pinealoblastoma
Wikipedia
American Journal of Neuroradiology . 16 (1): 157–65. PMID 7900586 . ^ de Jong MC, Kors WA, de Graaf P, Castelijns JA, Moll AC, Kivelä T (December 2015). ... PMID 10561222 . ^ de Jong MC, Kors WA, de Graaf P, Castelijns JA, Kivelä T, Moll AC (September 2014).
-
Giant Cell Arteritis
Wikipedia
Giant cell arteritis Other names Temporal arteritis, cranial arteritis, [1] Horton disease, [2] senile arteritis, [1] granulomatous arteritis [1] The arteries of the face and scalp Specialty Rheumatology , emergency medicine Symptoms Headache , pain over the temples, flu-like symptoms , double vision , difficulty opening the mouth [3] Complications Blindness , aortic dissection , aortic aneurysm , polymyalgia rheumatica [4] Usual onset Age greater than 50 [4] Causes Inflammation of the small blood vessels within the walls of larger arteries [4] Diagnostic method Based on symptoms and blood tests, confirmed by biopsy of the temporal artery [4] Differential diagnosis Takayasu arteritis , [5] stroke , primary amyloidosis [6] Treatment Steroids , bisphosphonates , proton-pump inhibitor [4] Prognosis Life expectancy (typically normal) [4] Frequency ~ 1 in 15,000 people a year (> 50 years old) [2] Giant cell arteritis ( GCA ), also called temporal arteritis , is an inflammatory disease of large blood vessels . [4] [7] Symptoms may include headache , pain over the temples, flu-like symptoms , double vision , and difficulty opening the mouth. [3] Complication can include blockage of the artery to the eye with resulting blindness , aortic dissection , and aortic aneurysm . [4] GCA is frequently associated with polymyalgia rheumatica . [4] The cause is unknown. [2] The underlying mechanism involves inflammation of the small blood vessels that occur within the walls of larger arteries. [4] This mainly affects arteries around the head and neck, though some in the chest may also be affected. [4] [8] Diagnosis is suspected based on symptoms, blood tests, and medical imaging , and confirmed by biopsy of the temporal artery . [4] However, in about 10% of people the temporal artery is normal. [4] Treatment is typically with high doses of steroids such as prednisone or prednisolone . [4] Once symptoms have resolved the dose is then decreased by about 15% per month. [4] Once a low dose is reached, the taper is slowed further over the subsequent year. [4] Other medications that may be recommended include bisphosphonates to prevent bone loss and a proton-pump inhibitor to prevent stomach problems. [4] It affects about 1 in 15,000 people over the age of 50 per year. [2] The condition typically only occurs in those over the age of 50, being most common among those in their 70s. [4] Females are more often affected than males. [4] Those of northern European descent are more commonly affected. [5] Life expectancy is typically normal. [4] The first description of the condition occurred in 1890. [1] Contents 1 Signs and symptoms 1.1 Associated conditions 2 Mechanism 3 Diagnosis 3.1 Physical exam 3.2 Laboratory tests 3.3 Biopsy 3.4 Medical imaging 4 Treatment 5 Epidemiology 6 Terminology 7 References 8 External links Signs and symptoms [ edit ] Common symptoms of giant cell arteritis include: bruits fever headache [9] tenderness and sensitivity on the scalp jaw claudication (pain in jaw when chewing) tongue claudication (pain in tongue when chewing) and necrosis [10] [11] reduced visual acuity (blurred vision) acute visual loss (sudden blindness) diplopia (double vision) acute tinnitus (ringing in the ears) polymyalgia rheumatica (in 50%) [12] The inflammation may affect blood supply to the eye ; blurred vision or sudden blindness may occur. ... Screening should be done on a case-by-case basis based on the signs and symptoms of people with GCA. [18] Mechanism [ edit ] The pathological mechanism is the result of an inflammatory cascade that is triggered by an as of yet determined cause resulting in dendritic cells in the vessel wall recruiting T cells and macrophages to form granulomatous infiltrates. [18] These infiltrates erode the middle and inner layers of the arterial tunica media leading to conditions such as aneurysm and dissection. [18] Activation of T helper 17 (Th17) cells involved with interleukin (IL) 6 , IL-17 , IL-21 and IL-23 play a critical part; specifically, Th17 activation leads to further activation of Th17 through IL-6 in a continuous, cyclic fashion. [18] This pathway is suppressed with glucocorticoids , [19] and more recently it has been found that IL-6 inhibitors also play a suppressive role. [18] Diagnosis [ edit ] Physical exam [ edit ] Palpation of the head reveals prominent temporal arteries with or without pulsation. [ citation needed ] The temporal area may be tender. [ citation needed ] Decreased pulses may be found throughout the body [ citation needed ] Evidence of ischemia may be noted on fundal exam. ... PMID 24988557 . ^ a b c Mackie, SL; Dejaco, C; Appenzeller, S; Camellino, D; Duftner, C; Gonzalez-Chiappe, S; Mahr, A; Mukhtyar, C; Reynolds, G; de Souza, AWS; Brouwer, E; Bukhari, M; Buttgereit, F; Byrne, D; Cid, MC; Cimmino, M; Direskeneli, H; Gilbert, K; Kermani, TA; Khan, A; Lanyon, P; Luqmani, R; Mallen, C; Mason, JC; Matteson, EL; Merkel, PA; Mollan, S; Neill, L; Sullivan, EO; Sandovici, M; Schmidt, WA; Watts, R; Whitlock, M; Yacyshyn, E; Ytterberg, S; Dasgupta, B (1 March 2020). ... PMID 16987903 . ^ Mackie, SL; Dejaco, C; Appenzeller, S; Camellino, D; Duftner, C; Gonzalez-Chiappe, S; Mahr, A; Mukhtyar, C; Reynolds, G; de Souza, AWS; Brouwer, E; Bukhari, M; Buttgereit, F; Byrne, D; Cid, MC; Cimmino, M; Direskeneli, H; Gilbert, K; Kermani, TA; Khan, A; Lanyon, P; Luqmani, R; Mallen, C; Mason, JC; Matteson, EL; Merkel, PA; Mollan, S; Neill, L; Sullivan, EO; Sandovici, M; Schmidt, WA; Watts, R; Whitlock, M; Yacyshyn, E; Ytterberg, S; Dasgupta, B (1 March 2020). ... OCLC 663444979 . ^ " giant cell arteritis " at Dorland's Medical Dictionary External links [ edit ] Mackie, SL; Dejaco, C; Appenzeller, S; Camellino, D; Duftner, C; Gonzalez-Chiappe, S; Mahr, A; Mukhtyar, C; Reynolds, G; de Souza, AWS; Brouwer, E; Bukhari, M; Buttgereit, F; Byrne, D; Cid, MC; Cimmino, M; Direskeneli, H; Gilbert, K; Kermani, TA; Khan, A; Lanyon, P; Luqmani, R; Mallen, C; Mason, JC; Matteson, EL; Merkel, PA; Mollan, S; Neill, L; Sullivan, EO; Sandovici, M; Schmidt, WA; Watts, R; Whitlock, M; Yacyshyn, E; Ytterberg, S; Dasgupta, B (1 March 2020).

-
Mycoplasma Hominis Infection
Wikipedia
Abstinence [8] Treatment [ edit ] Mycoplasmas have a triple-layered membrane and lack a cell wall. Commonly used antibiotics are generally ineffective because their efficacy is due to their ability to inhibit cell wall synthesis. Mycoplasmas are not affected by penicillins and other antibiotics that act on the cell wall. The growth of mycoplasmas in their host is inhibited by other broad-spectrum antibiotics. ... PMID 9421309 . ^ Goldenberg, RL; Andrews, WW; Goepfert, AR; Faye-Petersen, O; Cliver, SP; Carlo, WA; Hauth, JC (January 2008). "The Alabama Preterm Birth Study: umbilical cord blood Ureaplasma urealyticum and Mycoplasma hominis cultures in very preterm newborn infants" .
-
Fungal Meningitis
Wikipedia
There had been 30 fatalities. A black mold, Exserohilum rostratum , was found in 45 of these cases. ... External links [ edit ] Classification D MeSH : D016921 v t e Fungal infection and mesomycetozoea Superficial and cutaneous ( dermatomycosis ): Tinea = skin ; Piedra ( exothrix / endothrix ) = hair Ascomycota Dermatophyte ( Dermatophytosis ) By location Tinea barbae / tinea capitis Kerion Tinea corporis Ringworm Dermatophytids Tinea cruris Tinea manuum Tinea pedis (athlete's foot) Tinea unguium/onychomycosis White superficial onychomycosis Distal subungual onychomycosis Proximal subungual onychomycosis Tinea corporis gladiatorum Tinea faciei Tinea imbricata Tinea incognito Favus By organism Epidermophyton floccosum Microsporum canis Microsporum audouinii Trichophyton interdigitale/mentagrophytes Trichophyton tonsurans Trichophyton schoenleini Trichophyton rubrum Trichophyton verrucosum Other Hortaea werneckii Tinea nigra Piedraia hortae Black piedra Basidiomycota Malassezia furfur Tinea versicolor Pityrosporum folliculitis Trichosporon White piedra Subcutaneous , systemic , and opportunistic Ascomycota Dimorphic (yeast+mold) Onygenales Coccidioides immitis / Coccidioides posadasii Coccidioidomycosis Disseminated coccidioidomycosis Primary cutaneous coccidioidomycosis . Primary pulmonary coccidioidomycosis Histoplasma capsulatum Histoplasmosis Primary cutaneous histoplasmosis Primary pulmonary histoplasmosis Progressive disseminated histoplasmosis Histoplasma duboisii African histoplasmosis Lacazia loboi Lobomycosis Paracoccidioides brasiliensis Paracoccidioidomycosis Other Blastomyces dermatitidis Blastomycosis North American blastomycosis South American blastomycosis Sporothrix schenckii Sporotrichosis Talaromyces marneffei Talaromycosis Yeast -like Candida albicans Candidiasis Oral Esophageal Vulvovaginal Chronic mucocutaneous Antibiotic candidiasis Candidal intertrigo Candidal onychomycosis Candidal paronychia Candidid Diaper candidiasis Congenital cutaneous candidiasis Perianal candidiasis Systemic candidiasis Erosio interdigitalis blastomycetica C. auris C. glabrata C. lusitaniae C. tropicalis Pneumocystis jirovecii Pneumocystosis Pneumocystis pneumonia Mold -like Aspergillus Aspergillosis Aspergilloma Allergic bronchopulmonary aspergillosis Primary cutaneous aspergillosis Exophiala jeanselmei Eumycetoma Fonsecaea pedrosoi / Fonsecaea compacta / Phialophora verrucosa Chromoblastomycosis Geotrichum candidum Geotrichosis Pseudallescheria boydii Allescheriasis Basidiomycota Cryptococcus neoformans Cryptococcosis Trichosporon spp Trichosporonosis Zygomycota ( Zygomycosis ) Mucorales ( Mucormycosis ) Rhizopus oryzae Mucor indicus Lichtheimia corymbifera Syncephalastrum racemosum Apophysomyces variabilis Entomophthorales ( Entomophthoramycosis ) Basidiobolus ranarum Basidiobolomycosis Conidiobolus coronatus / Conidiobolus incongruus Conidiobolomycosis Microsporidia ( Microsporidiosis ) Enterocytozoon bieneusi / Encephalitozoon intestinalis Mesomycetozoea Rhinosporidium seeberi Rhinosporidiosis Ungrouped Alternariosis Fungal folliculitis Fusarium Fusariosis Granuloma gluteale infantum Hyalohyphomycosis Otomycosis Phaeohyphomycosis v t e Meningitis and other diseases of meninges Meningitis Arachnoiditis Bacterial Tuberculous Haemophilus Pneumococcal Viral Herpesviral Fungal Cryptococcal Aseptic Drug-induced Other Meningoencephalitis

-
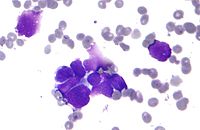
Nuclear Moulding
Wikipedia
In histo pathology , nuclear moulding , also nuclear molding , is conformity of adjacent cell nuclei to one another. [1] It is a feature of small cell carcinomas and particularly useful for differentiation of small cell and non-small cell carcinomas, i.e. adenocarcinoma and squamous carcinoma . [2] See also [ edit ] Merkel cell carcinoma Lung cancer References [ edit ] ^ "http://www.vet.ohio-state.edu/assets/courses/vm618/gloss/glossary.html" .
-
Tinea Faciei
Wikipedia
External links [ edit ] Classification D ICD - 10 : B35.8 ICD - 9-CM : 110.8 v t e Fungal infection and mesomycetozoea Superficial and cutaneous ( dermatomycosis ): Tinea = skin ; Piedra ( exothrix / endothrix ) = hair Ascomycota Dermatophyte ( Dermatophytosis ) By location Tinea barbae / tinea capitis Kerion Tinea corporis Ringworm Dermatophytids Tinea cruris Tinea manuum Tinea pedis (athlete's foot) Tinea unguium/onychomycosis White superficial onychomycosis Distal subungual onychomycosis Proximal subungual onychomycosis Tinea corporis gladiatorum Tinea faciei Tinea imbricata Tinea incognito Favus By organism Epidermophyton floccosum Microsporum canis Microsporum audouinii Trichophyton interdigitale/mentagrophytes Trichophyton tonsurans Trichophyton schoenleini Trichophyton rubrum Trichophyton verrucosum Other Hortaea werneckii Tinea nigra Piedraia hortae Black piedra Basidiomycota Malassezia furfur Tinea versicolor Pityrosporum folliculitis Trichosporon White piedra Subcutaneous , systemic , and opportunistic Ascomycota Dimorphic (yeast+mold) Onygenales Coccidioides immitis / Coccidioides posadasii Coccidioidomycosis Disseminated coccidioidomycosis Primary cutaneous coccidioidomycosis . Primary pulmonary coccidioidomycosis Histoplasma capsulatum Histoplasmosis Primary cutaneous histoplasmosis Primary pulmonary histoplasmosis Progressive disseminated histoplasmosis Histoplasma duboisii African histoplasmosis Lacazia loboi Lobomycosis Paracoccidioides brasiliensis Paracoccidioidomycosis Other Blastomyces dermatitidis Blastomycosis North American blastomycosis South American blastomycosis Sporothrix schenckii Sporotrichosis Talaromyces marneffei Talaromycosis Yeast -like Candida albicans Candidiasis Oral Esophageal Vulvovaginal Chronic mucocutaneous Antibiotic candidiasis Candidal intertrigo Candidal onychomycosis Candidal paronychia Candidid Diaper candidiasis Congenital cutaneous candidiasis Perianal candidiasis Systemic candidiasis Erosio interdigitalis blastomycetica C. auris C. glabrata C. lusitaniae C. tropicalis Pneumocystis jirovecii Pneumocystosis Pneumocystis pneumonia Mold -like Aspergillus Aspergillosis Aspergilloma Allergic bronchopulmonary aspergillosis Primary cutaneous aspergillosis Exophiala jeanselmei Eumycetoma Fonsecaea pedrosoi / Fonsecaea compacta / Phialophora verrucosa Chromoblastomycosis Geotrichum candidum Geotrichosis Pseudallescheria boydii Allescheriasis Basidiomycota Cryptococcus neoformans Cryptococcosis Trichosporon spp Trichosporonosis Zygomycota ( Zygomycosis ) Mucorales ( Mucormycosis ) Rhizopus oryzae Mucor indicus Lichtheimia corymbifera Syncephalastrum racemosum Apophysomyces variabilis Entomophthorales ( Entomophthoramycosis ) Basidiobolus ranarum Basidiobolomycosis Conidiobolus coronatus / Conidiobolus incongruus Conidiobolomycosis Microsporidia ( Microsporidiosis ) Enterocytozoon bieneusi / Encephalitozoon intestinalis Mesomycetozoea Rhinosporidium seeberi Rhinosporidiosis Ungrouped Alternariosis Fungal folliculitis Fusarium Fusariosis Granuloma gluteale infantum Hyalohyphomycosis Otomycosis Phaeohyphomycosis This infection-related cutaneous condition article is a stub .

-
Coronary Artery Anomaly
Wikipedia
Coronary arteries are identified according to the myocardial territory they feed: 1) the LAD supplies the anterior interventricular septum and anterior left ventricular free wall; 2) the LCx supplies the posterolateral left ventricular free wall; 3) the RCA supplies the right ventricular free wall; In fact, despite a certain degree of variability in coronary artery anatomy among individuals, there is greater consistency in the regions of the heart that are supplied by the different coronary arteries. The posterior descending artery , providing blood flow to the infero-posterior wall of the heart, originates from the RCA in 70-90% of individuals (“right coronary dominance”), whereas in 10-15% cases it originates from the LCx (“left coronary dominance”). ... Indeed, the main feature responsible for adverse outcomes is the “intramural” course (sometimes improperly referred to as inter-arterial) characterized by an acute ostial angulation (tangential course), “slit-like” ostium (compressed inside the aortic wall), and a proximal or initial section penetrating into the aortic tunica media (coronary arteries normally take off at a 90 degree angle) with subsequent course reaching the “correct” side of the heart. ... Some cases are congenital/idiopathic, but most are secondary to atherosclerosis or Kawasaki disease (an immuno-inflammatory disease especially targeting coronary vessels wall). Potential complications include localized thrombosis, distal embolization, rupture, or late lipid deposits. ... Surgery consists of “unroofing” or denudation of the intramural coronary segment from the aortic wall: this approach is currently the gold standard.
-
White Piedra
Wikipedia
External links [ edit ] Classification D ICD - 10 : B36.2 ICD - 9-CM : 111.2 MeSH : D010854 DiseasesDB : 31871 DermAtlas 2062238337 v t e Fungal infection and mesomycetozoea Superficial and cutaneous ( dermatomycosis ): Tinea = skin ; Piedra ( exothrix / endothrix ) = hair Ascomycota Dermatophyte ( Dermatophytosis ) By location Tinea barbae / tinea capitis Kerion Tinea corporis Ringworm Dermatophytids Tinea cruris Tinea manuum Tinea pedis (athlete's foot) Tinea unguium/onychomycosis White superficial onychomycosis Distal subungual onychomycosis Proximal subungual onychomycosis Tinea corporis gladiatorum Tinea faciei Tinea imbricata Tinea incognito Favus By organism Epidermophyton floccosum Microsporum canis Microsporum audouinii Trichophyton interdigitale/mentagrophytes Trichophyton tonsurans Trichophyton schoenleini Trichophyton rubrum Trichophyton verrucosum Other Hortaea werneckii Tinea nigra Piedraia hortae Black piedra Basidiomycota Malassezia furfur Tinea versicolor Pityrosporum folliculitis Trichosporon White piedra Subcutaneous , systemic , and opportunistic Ascomycota Dimorphic (yeast+mold) Onygenales Coccidioides immitis / Coccidioides posadasii Coccidioidomycosis Disseminated coccidioidomycosis Primary cutaneous coccidioidomycosis . Primary pulmonary coccidioidomycosis Histoplasma capsulatum Histoplasmosis Primary cutaneous histoplasmosis Primary pulmonary histoplasmosis Progressive disseminated histoplasmosis Histoplasma duboisii African histoplasmosis Lacazia loboi Lobomycosis Paracoccidioides brasiliensis Paracoccidioidomycosis Other Blastomyces dermatitidis Blastomycosis North American blastomycosis South American blastomycosis Sporothrix schenckii Sporotrichosis Talaromyces marneffei Talaromycosis Yeast -like Candida albicans Candidiasis Oral Esophageal Vulvovaginal Chronic mucocutaneous Antibiotic candidiasis Candidal intertrigo Candidal onychomycosis Candidal paronychia Candidid Diaper candidiasis Congenital cutaneous candidiasis Perianal candidiasis Systemic candidiasis Erosio interdigitalis blastomycetica C. auris C. glabrata C. lusitaniae C. tropicalis Pneumocystis jirovecii Pneumocystosis Pneumocystis pneumonia Mold -like Aspergillus Aspergillosis Aspergilloma Allergic bronchopulmonary aspergillosis Primary cutaneous aspergillosis Exophiala jeanselmei Eumycetoma Fonsecaea pedrosoi / Fonsecaea compacta / Phialophora verrucosa Chromoblastomycosis Geotrichum candidum Geotrichosis Pseudallescheria boydii Allescheriasis Basidiomycota Cryptococcus neoformans Cryptococcosis Trichosporon spp Trichosporonosis Zygomycota ( Zygomycosis ) Mucorales ( Mucormycosis ) Rhizopus oryzae Mucor indicus Lichtheimia corymbifera Syncephalastrum racemosum Apophysomyces variabilis Entomophthorales ( Entomophthoramycosis ) Basidiobolus ranarum Basidiobolomycosis Conidiobolus coronatus / Conidiobolus incongruus Conidiobolomycosis Microsporidia ( Microsporidiosis ) Enterocytozoon bieneusi / Encephalitozoon intestinalis Mesomycetozoea Rhinosporidium seeberi Rhinosporidiosis Ungrouped Alternariosis Fungal folliculitis Fusarium Fusariosis Granuloma gluteale infantum Hyalohyphomycosis Otomycosis Phaeohyphomycosis This condition of the skin appendages article is a stub .

-
Zygomycosis
Wikipedia
Mucormycosis Periorbital fungal infection known as mucormycosis, or phycomycosis Specialty Infectious disease Zygomycosis is the broadest term to refer to infections caused by bread mold fungi of the zygomycota phylum. However, because zygomycota has been identified as polyphyletic , and is not included in modern fungal classification systems, the diseases that zygomycosis can refer to are better called by their specific names: mucormycosis [1] (after Mucorales ), phycomycosis [2] (after Phycomycetes ) and basidiobolomycosis (after Basidiobolus ). [3] These rare yet serious and potentially life-threatening fungal infections usually affect the face or oropharyngeal (nose and mouth) cavity. [4] Zygomycosis type infections are most often caused by common fungi found in soil and decaying vegetation. ... External links [ edit ] Classification D ICD - 10 : B46 ICD - 9-CM : 117.7 MeSH : D020096 DiseasesDB : 31329 External resources MedlinePlus : 000649 eMedicine : med/1513 med/2026 oph/225 ped/1488 v t e Fungal infection and mesomycetozoea Superficial and cutaneous ( dermatomycosis ): Tinea = skin ; Piedra ( exothrix / endothrix ) = hair Ascomycota Dermatophyte ( Dermatophytosis ) By location Tinea barbae / tinea capitis Kerion Tinea corporis Ringworm Dermatophytids Tinea cruris Tinea manuum Tinea pedis (athlete's foot) Tinea unguium/onychomycosis White superficial onychomycosis Distal subungual onychomycosis Proximal subungual onychomycosis Tinea corporis gladiatorum Tinea faciei Tinea imbricata Tinea incognito Favus By organism Epidermophyton floccosum Microsporum canis Microsporum audouinii Trichophyton interdigitale/mentagrophytes Trichophyton tonsurans Trichophyton schoenleini Trichophyton rubrum Trichophyton verrucosum Other Hortaea werneckii Tinea nigra Piedraia hortae Black piedra Basidiomycota Malassezia furfur Tinea versicolor Pityrosporum folliculitis Trichosporon White piedra Subcutaneous , systemic , and opportunistic Ascomycota Dimorphic (yeast+mold) Onygenales Coccidioides immitis / Coccidioides posadasii Coccidioidomycosis Disseminated coccidioidomycosis Primary cutaneous coccidioidomycosis . Primary pulmonary coccidioidomycosis Histoplasma capsulatum Histoplasmosis Primary cutaneous histoplasmosis Primary pulmonary histoplasmosis Progressive disseminated histoplasmosis Histoplasma duboisii African histoplasmosis Lacazia loboi Lobomycosis Paracoccidioides brasiliensis Paracoccidioidomycosis Other Blastomyces dermatitidis Blastomycosis North American blastomycosis South American blastomycosis Sporothrix schenckii Sporotrichosis Talaromyces marneffei Talaromycosis Yeast -like Candida albicans Candidiasis Oral Esophageal Vulvovaginal Chronic mucocutaneous Antibiotic candidiasis Candidal intertrigo Candidal onychomycosis Candidal paronychia Candidid Diaper candidiasis Congenital cutaneous candidiasis Perianal candidiasis Systemic candidiasis Erosio interdigitalis blastomycetica C. auris C. glabrata C. lusitaniae C. tropicalis Pneumocystis jirovecii Pneumocystosis Pneumocystis pneumonia Mold -like Aspergillus Aspergillosis Aspergilloma Allergic bronchopulmonary aspergillosis Primary cutaneous aspergillosis Exophiala jeanselmei Eumycetoma Fonsecaea pedrosoi / Fonsecaea compacta / Phialophora verrucosa Chromoblastomycosis Geotrichum candidum Geotrichosis Pseudallescheria boydii Allescheriasis Basidiomycota Cryptococcus neoformans Cryptococcosis Trichosporon spp Trichosporonosis Zygomycota ( Zygomycosis ) Mucorales ( Mucormycosis ) Rhizopus oryzae Mucor indicus Lichtheimia corymbifera Syncephalastrum racemosum Apophysomyces variabilis Entomophthorales ( Entomophthoramycosis ) Basidiobolus ranarum Basidiobolomycosis Conidiobolus coronatus / Conidiobolus incongruus Conidiobolomycosis Microsporidia ( Microsporidiosis ) Enterocytozoon bieneusi / Encephalitozoon intestinalis Mesomycetozoea Rhinosporidium seeberi Rhinosporidiosis Ungrouped Alternariosis Fungal folliculitis Fusarium Fusariosis Granuloma gluteale infantum Hyalohyphomycosis Otomycosis Phaeohyphomycosis

-
Paracoccidioidomycosis
Wikipedia
Classic lesions are superficial painful granular ulcers , with small spots of bleeding. [11] Cause [ edit ] Paracoccidioidomycosis is caused by two species of fungi that can exist as a mold or yeast depending on temperature , P. brasiliensis and P. lutzii. ... Histopathological study with Gomori methenamine silver (GMS) stain or hematoxylin and eosin ( H&E ) stain revealing large yeast cells with translucent cell walls with multiple buds. [10] In the juvenile form, lung abnormalities are shown in high-resolution CT scans of the lungs, whereas in the chronic form plain X-rays may show interstitial and alveolar infiltrates in the central and lower lung fields. [10] Culture of P. brasiliensis takes between 20–30 days, requiring multiple samples and culture media. ... Melhoramentos (in Portuguese), São Paulo: 98 pages External links [ edit ] Classification D ICD - 10 : B41 ICD - 9-CM : 116.1 MeSH : D010229 DiseasesDB : 29815 External resources eMedicine : med/1731 Orphanet : 73260 v t e Fungal infection and mesomycetozoea Superficial and cutaneous ( dermatomycosis ): Tinea = skin ; Piedra ( exothrix / endothrix ) = hair Ascomycota Dermatophyte ( Dermatophytosis ) By location Tinea barbae / tinea capitis Kerion Tinea corporis Ringworm Dermatophytids Tinea cruris Tinea manuum Tinea pedis (athlete's foot) Tinea unguium/onychomycosis White superficial onychomycosis Distal subungual onychomycosis Proximal subungual onychomycosis Tinea corporis gladiatorum Tinea faciei Tinea imbricata Tinea incognito Favus By organism Epidermophyton floccosum Microsporum canis Microsporum audouinii Trichophyton interdigitale/mentagrophytes Trichophyton tonsurans Trichophyton schoenleini Trichophyton rubrum Trichophyton verrucosum Other Hortaea werneckii Tinea nigra Piedraia hortae Black piedra Basidiomycota Malassezia furfur Tinea versicolor Pityrosporum folliculitis Trichosporon White piedra Subcutaneous , systemic , and opportunistic Ascomycota Dimorphic (yeast+mold) Onygenales Coccidioides immitis / Coccidioides posadasii Coccidioidomycosis Disseminated coccidioidomycosis Primary cutaneous coccidioidomycosis . Primary pulmonary coccidioidomycosis Histoplasma capsulatum Histoplasmosis Primary cutaneous histoplasmosis Primary pulmonary histoplasmosis Progressive disseminated histoplasmosis Histoplasma duboisii African histoplasmosis Lacazia loboi Lobomycosis Paracoccidioides brasiliensis Paracoccidioidomycosis Other Blastomyces dermatitidis Blastomycosis North American blastomycosis South American blastomycosis Sporothrix schenckii Sporotrichosis Talaromyces marneffei Talaromycosis Yeast -like Candida albicans Candidiasis Oral Esophageal Vulvovaginal Chronic mucocutaneous Antibiotic candidiasis Candidal intertrigo Candidal onychomycosis Candidal paronychia Candidid Diaper candidiasis Congenital cutaneous candidiasis Perianal candidiasis Systemic candidiasis Erosio interdigitalis blastomycetica C. auris C. glabrata C. lusitaniae C. tropicalis Pneumocystis jirovecii Pneumocystosis Pneumocystis pneumonia Mold -like Aspergillus Aspergillosis Aspergilloma Allergic bronchopulmonary aspergillosis Primary cutaneous aspergillosis Exophiala jeanselmei Eumycetoma Fonsecaea pedrosoi / Fonsecaea compacta / Phialophora verrucosa Chromoblastomycosis Geotrichum candidum Geotrichosis Pseudallescheria boydii Allescheriasis Basidiomycota Cryptococcus neoformans Cryptococcosis Trichosporon spp Trichosporonosis Zygomycota ( Zygomycosis ) Mucorales ( Mucormycosis ) Rhizopus oryzae Mucor indicus Lichtheimia corymbifera Syncephalastrum racemosum Apophysomyces variabilis Entomophthorales ( Entomophthoramycosis ) Basidiobolus ranarum Basidiobolomycosis Conidiobolus coronatus / Conidiobolus incongruus Conidiobolomycosis Microsporidia ( Microsporidiosis ) Enterocytozoon bieneusi / Encephalitozoon intestinalis Mesomycetozoea Rhinosporidium seeberi Rhinosporidiosis Ungrouped Alternariosis Fungal folliculitis Fusarium Fusariosis Granuloma gluteale infantum Hyalohyphomycosis Otomycosis PhaeohyphomycosisIFNG, IL10, TNF, IL4, CTLA4, S100A10, HSPD1, CD40LG, EXOSC3, HSPA14, TPI1, VDR, CHST3, TUBA1B, IL37, PYCARD, CD209, NLRP3, RBM45, TLR5, IL23A, YTHDF1, NLN, CLEC7A, LPAL2, IL33, OPN4, APOA2, SFTPD, TLR3, ICAM1, TSPO, CD28, CHRM3, FCGR2A, G6PD, GPI, GSR, HLA-DRB1, IL12B, STAT4, IL12RB1, IL17A, LGALS3, NOS2, NOTCH1, OPRM1, STS, STAT3, IL23R

-
Blight
Wikipedia
Several notable examples are: Late blight of potato , caused by the water mold Phytophthora infestans (Mont.) de Bary, the disease which led to the Great Irish Famine Southern corn leaf blight, caused by the fungus Cochliobolus heterostrophus (Drechs.) ... For example, Colletotrichum blight is named after the fungus Colletotrichum capsici , and Phytophthora blight is named after the water mold Phytophthora parasitica . [6] Gallery [ edit ] Chestnut blight Brown felt blight Potato late blight Fire blight appletree fruit References [ edit ] ^ Agrios, George N. 2005.
-
Crayfish Plague
Wikipedia
Water mold disease Crayfish plague Mycelial filaments from Aphanomyces astaci on membranes of Pacifastacus leniusculus Scientific classification Clade : SAR Phylum: Oomycota Order: Saprolegniales Family: Leptolegniaceae Genus: Aphanomyces Species: A. astaci Binomial name Aphanomyces astaci Schikora , 1906 [1] Crayfish plague ( Aphanomyces astaci ) is a water mold that infects crayfish , most notably the European Astacus which dies within a few weeks of being infected.

-
Talaromycosis
Wikipedia
External links [ edit ] Classification D ICD - 10 : B48.4 ICD - 9-CM : 117.3 DiseasesDB : 9802 v t e Fungal infection and mesomycetozoea Superficial and cutaneous ( dermatomycosis ): Tinea = skin ; Piedra ( exothrix / endothrix ) = hair Ascomycota Dermatophyte ( Dermatophytosis ) By location Tinea barbae / tinea capitis Kerion Tinea corporis Ringworm Dermatophytids Tinea cruris Tinea manuum Tinea pedis (athlete's foot) Tinea unguium/onychomycosis White superficial onychomycosis Distal subungual onychomycosis Proximal subungual onychomycosis Tinea corporis gladiatorum Tinea faciei Tinea imbricata Tinea incognito Favus By organism Epidermophyton floccosum Microsporum canis Microsporum audouinii Trichophyton interdigitale/mentagrophytes Trichophyton tonsurans Trichophyton schoenleini Trichophyton rubrum Trichophyton verrucosum Other Hortaea werneckii Tinea nigra Piedraia hortae Black piedra Basidiomycota Malassezia furfur Tinea versicolor Pityrosporum folliculitis Trichosporon White piedra Subcutaneous , systemic , and opportunistic Ascomycota Dimorphic (yeast+mold) Onygenales Coccidioides immitis / Coccidioides posadasii Coccidioidomycosis Disseminated coccidioidomycosis Primary cutaneous coccidioidomycosis . Primary pulmonary coccidioidomycosis Histoplasma capsulatum Histoplasmosis Primary cutaneous histoplasmosis Primary pulmonary histoplasmosis Progressive disseminated histoplasmosis Histoplasma duboisii African histoplasmosis Lacazia loboi Lobomycosis Paracoccidioides brasiliensis Paracoccidioidomycosis Other Blastomyces dermatitidis Blastomycosis North American blastomycosis South American blastomycosis Sporothrix schenckii Sporotrichosis Talaromyces marneffei Talaromycosis Yeast -like Candida albicans Candidiasis Oral Esophageal Vulvovaginal Chronic mucocutaneous Antibiotic candidiasis Candidal intertrigo Candidal onychomycosis Candidal paronychia Candidid Diaper candidiasis Congenital cutaneous candidiasis Perianal candidiasis Systemic candidiasis Erosio interdigitalis blastomycetica C. auris C. glabrata C. lusitaniae C. tropicalis Pneumocystis jirovecii Pneumocystosis Pneumocystis pneumonia Mold -like Aspergillus Aspergillosis Aspergilloma Allergic bronchopulmonary aspergillosis Primary cutaneous aspergillosis Exophiala jeanselmei Eumycetoma Fonsecaea pedrosoi / Fonsecaea compacta / Phialophora verrucosa Chromoblastomycosis Geotrichum candidum Geotrichosis Pseudallescheria boydii Allescheriasis Basidiomycota Cryptococcus neoformans Cryptococcosis Trichosporon spp Trichosporonosis Zygomycota ( Zygomycosis ) Mucorales ( Mucormycosis ) Rhizopus oryzae Mucor indicus Lichtheimia corymbifera Syncephalastrum racemosum Apophysomyces variabilis Entomophthorales ( Entomophthoramycosis ) Basidiobolus ranarum Basidiobolomycosis Conidiobolus coronatus / Conidiobolus incongruus Conidiobolomycosis Microsporidia ( Microsporidiosis ) Enterocytozoon bieneusi / Encephalitozoon intestinalis Mesomycetozoea Rhinosporidium seeberi Rhinosporidiosis Ungrouped Alternariosis Fungal folliculitis Fusarium Fusariosis Granuloma gluteale infantum Hyalohyphomycosis Otomycosis Phaeohyphomycosis
-
Downy Mildew
Wikipedia
Upon closer inspection, a purple-brown mold (see arrow) becomes apparent. Small spores shaped like footballs can be observed among the mold with a 10x hand lens. ... Tufts of grayish to pale-colored sporangiophores on the underside of leaves easily distinguish the infection from other foliar diseases. [11] The disease is often controlled using the fungicides mancozeb , maneb , or zineb . [10] Spinach [ edit ] Downy mildew on spinach is caused by Peronospora effusa, an oomycete pathogen that poses a challenge to spinach production worldwide, especially in organic production. [12] Sunflowers [ edit ] Plasmopara halstedii infects sunflowers , producing oospores which can remain dormant in the soil for many years. [13] See also [ edit ] Blue mold (of tobacco plants) Peronosporaceae (with a list of the downy mildew genera) References [ edit ] ^ NCBI-Taxonomy – ncbi.nlm.nih.gov ^ HYP3 – ncbi.nlm.nih.gov ^ Schilder, Annemiek.

-
Food Poisoning
Mayo Clinic
Bacteria that carry or make toxins. Molds that make toxins. Understanding terms The term "food poisoning" is commonly used to describe all foodborne illnesses. ... Throw out moldy food. Throw out any baked foods with mold. Throw out moldy soft fruits and vegetables, such as tomatoes, berries or peaches. And throw away any nuts or nut products with mold. You can trim away mold from firm foods with low moisture, such as carrots, bell peppers and hard cheeses. ... Make a cleaning solution of 1 tablespoon (15 milliliters) of baking soda and 1 quart (0.9 liters) of water. Clean visible mold in the refrigerator or on the door seals.
- Heck's Disease Wikipedia












