-
Migrainous Infarction
Wikipedia
CS1 maint: DOI inactive as of January 2021 ( link ) ^ a b c d e Viana, M.; Linde, M.; Sances, G.; Ghiotto, N.; Guaschino, E.; Allena, M.; Terrazzino, S.; Nappi, G.; Goadsby, P. ... S2CID 6290227 . ^ Ameri, A.; Bousser, M. G. (1992-02-01). "Cerebral Venous Thrombosis" . ... PMC 1739108 . PMID 15201354 . ^ a b c D'Andrea, G.; Toldo, M.; Cananzi, A.; Ferro-Milone, F. (1984-03-01). ... ISSN 0006-8950 . PMID 8453456 . ^ Kreling, G. A. D.; de Almeida, N. R.; dos Santos, P. ... PMID 28740841 . ^ Lee, H.; Whitman, G. T.; Lim, J. G.; Yi, S. D.; Cho, Y.
-
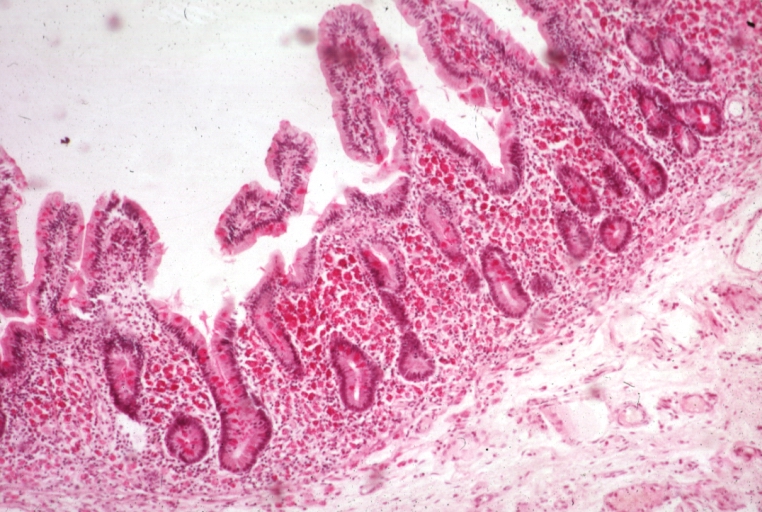
Malabsorption
Wikipedia
A typical Western diet ingested by an adult in one day includes approximately 100 g of fat, 400 g of carbohydrate, 100 g of protein, 2 L of fluid, and the required sodium , potassium , chloride , calcium , vitamins , and other elements. [ citation needed ] Salivary , gastric , intestinal , hepatic , and pancreatic secretions add an additional 7–8 L of protein-, lipid-, and electrolyte-containing fluid to intestinal contents. This massive load is reduced by the small and large intestines to less than 200 g of stool that contains less than 8 g of fat, 1–2 g of nitrogen, and less than 20 mmol each of Na + , K + , Cl – , HCO 3 – , Ca 2+ , or Mg 2+ . ... PMID 12192177 . S2CID 10373517 . ^ Gasbarrini G, Frisono M: Critical evaluation of malabsorption tests; in Dobrilla G, Bertaccini G (1986). Langman G (ed.). Problems and Controversies in Gastroenterology . ... PMID 7350049 . ^ a b c Thomas P, Forbes A, Green J, Howdle P, Long R, Playford R, Sheridan M, Stevens R, Valori R, Walters J, Addison G, Hill P, Brydon G (2003). "Guidelines for the investigation of chronic diarrhoea, 2nd edition" .SLC46A1, CFTR, CBLIF, SI, MTTP, NEUROG3, ARX, SLC5A1, PCSK1, SLC6A19, RFX6, PEX14, PEX6, TCF3, PEX10, TERC, TERT, TGFB1, TGFBR2, TLR4, KDM6A, CLIP2, STAT4, WFS1, XRCC4, KMT2D, KLRC4, PEX3, RFXANK, PEX11B, BAZ1B, STX1A, AKR1D1, SRP54, RFC2, PIK3CA, PEX13, PIK3R1, PMS1, PMS2, POLG, PEX19, PEX5, RFX5, ABCB4, RFXAP, RMRP, RPS20, SAA1, PEX12, PEX16, SLC2A2, SLCO2A1, RECQL4, AGA, ADAMTS3, USB1, SLC39A4, NHP2, PEX26, LRRC8A, TRMT5, SEMA4A, CYBC1, EFL1, FAT4, CTC1, GTF2IRD1, HSD3B7, CDCA7, DNAJC21, CCBE1, IL23R, UBR1, UBAC2, CISD2, NCF1, NOP10, SLC29A3, WRAP53, NSUN2, LPIN2, PEX1, HYOU1, SRCAP, SPINK5, CLCA4, FAN1, PMPCA, VPS13A, TINF2, TBL2, MLH3, BLNK, SH3KBP1, FOXP3, SBDS, DCTN4, RTEL1, ERAP1, ZBTB24, PEX2, ENPP1, DNMT3B, ELN, ERCC2, F5, FLNA, GLA, MSH6, GTF2I, HBB, HELLS, HLA-B, HLA-DRB1, PARN, IGHM, IGLL1, IL10, IL12A, IRF5, JAK2, KRAS, TYMP, DMP1, LIMK1, DKC1, AK2, APC, FAS, ATP7A, B2M, BMPR1A, BTK, C4A, CAV1, CD79A, CD79B, CCR1, CCR6, CCN2, CTNNB1, CYBA, CYBB, CYP27A1, CD55, LIG4, HPGD, IL12A-AS1, TRNW, COX1, COX2, COX3, ND1, MYD88, ND5, ND6, TRNE, MPI, TRNS2, TRNF, TRNH, TRNK, TRNL1, TRNQ, TRNS1, MSH2, ND4, MLH1, MEFV, NCF4, OCRL, EPCAM, NCF2, CIITA, CUBN, SLC2A5, APOB, SAR1B, TNF, TGM2, ACE, AGT, ACAD8, AMN, PTH, GCG, MMUT, PAEP, MYO5B, HT, ATP4A, MYLK, TPH2, PLF, PYY, HAMP, NLRP3, ATP12A, COX4I2, PNLIP, OR10A4, CD40, PANK2, REXO1L1P, CD36, ATP8B1, CCK, TPH1, CLDN4, PDP1, UCP2, EZR, LEP, LCT, TH, KIT, KDR, DGAT1, RAB11A, NRP1, CLDN2, MT1B, NCOA2, SLC10A2, MGLL, GSR, GH1, PTPN22, CNNM4, FGR, FAT1, FABP1, MTR, EXOSC3, TTR, S100A10, RNPEP, MLXIPL
-
Benign Familial Neonatal Seizures
Wikipedia
S2CID 37406352 . ^ Miraglia del Giudice E, Coppola G, Scuccimarra G, Cirillo G, Bellini G, Pascotto A (2000). ... PMID 11175290 . ^ a b Castaldo P, del Giudice E, Coppola G, Pascotto A, Annunziato L, Taglialatela M (2002). ... Neurology . 63 (1): 57–65. doi : 10.1212/01.wnl.0000132979.08394.6d . PMID 15249611 . ^ de Haan G, Pinto D, Carton D, Bader A, Witte J, Peters E, van Erp G, Vandereyken W, Boezeman E, Wapenaar M, Boon P, Halley D, Koeleman B, Lindhout D (2006). ... PMID 15178210 . S2CID 36912785 . ^ a b Coppola G, Castaldo P, Miraglia del Giudice E, Bellini G, Galasso F, Soldovieri M, Anzalone L, Sferro C, Annunziato L, Pascotto A, Taglialatela M (2003). ... PMID 10852552 . ^ Concolino D, Iembo M, Rossi E, Giglio S, Coppola G, Miraglia Del Giudice E, Strisciuglio P (2002).
-
Systemic Lupus Erythematosus, Susceptibility To, 12
OMIM
Homozygotes for the A allele of rs13277113 had levels of BLK mRNA expression that were approximately 50% of those of homozygotes for the G allele. The expression of the C8ORF13 gene also correlated with the rs13277113 SNP, but in the opposite direction. The A allele was associated with higher expression of C8ORF13, whereas the G allele was significantly associated with lower expression. A/G heterozygotes had intermediate levels of expression of both genes.
-
Blue Cone Monochromacy
Wikipedia
PMID 20220053 . ^ a b c d e Alpern, M; Falls, H F; Lee, G B (1960). "The enigma of typical total monochromacy". ... PMC 2676201 . PMID 19421413 . ^ a b c d e f g Michaelides, M; Johnson, S; Simunovic, M P; Bradshaw, K; Holder, G; Mollon, J D; Moore, A T; Hunt, D M (2005). ... Ophthalmol . 242 (9): 729–735. doi : 10.1007/s00417-004-0921-z . PMID 15069569 . ^ a b c d e f g h i Nathans, J; Davenport, C M; Maumenee, I H; Lewis, R A; Hejtmancik, J F; Litt, M; Lovrien, E; Weleber, R; Bachynski, B; Zwas, F; Klingaman, R; Fishman, G (1989). ... PMID 21267011 . ^ a b c Gardner, J C; Webb, T R; Kanuga, N; Robson, A G; Holder, G E; Stockman, A; Ripamonti, C; Ebenezer, N D; Ogun, O; Devery, S; Wright, G A; Maher, E R; Cheetham, M E; Moore, A T; Michaelides, M; Hardcastle, A J (2010). ... PMID 8666378 . ^ a b c d Gardner, J C; Liew, G; Quan, Y H; Ermetal, B; Ueyama, H; Davidson, A E; Schwarz, N; Kanuga, N; Chana, R; Maher, E; Webster, A R; Holder, G E; Robson, A G; Cheetham, M E; Liebelt, J; Ruddle, J B; Moore, A T; Michaelides, M; Hardcastle, A J (2014).
-
Large For Gestational Age
Wikipedia
These generally involve trying to turn the shoulders into the oblique, using suprapubic pressure to disimpact the anterior shoulder from above the pubic symphysis, or delivering the posterior arm first. [8] If these do not resolve the situation, the provider may intentionally snap the baby's clavicle (bone that holds shoulder in place) in a procedure called cleidotomy in order to displace the shoulder and allow the child to be delivered. [9] [10] Other methods to deliver the baby as a last resort when all else have failed are the Zavanelli maneuver and symphysiotomy. [9] [10] The Zavanelli maneuver involves flexing and pushing the fetal head back into the birth canal, and an emergency cesarean section is then performed. [10] Symphysiotomy allows childbirth by surgically dividing the pubic bone to widen the pelvis and it is performed after a failed Zavanelli maneuver. [10] Newborns with shoulder dystocia are at risk of temporary or permanent nerve damage to the baby's arm, or other injuries such as humeral fracture. [8] In non-diabetic women, shoulder dystocia happens 0.65% of the time in babies that weigh less than 8 pounds 13 ounces (4,000 g), 6.7% of the time in babies that weigh 8 pounds 13 ounces (4,000 g) to 9 pounds 15 ounces (4,500 g), and 14.5% of the time in babies that weigh more than 9 pounds 15 ounces (4,500 g). [11] In diabetic women, shoulder dystocia happens 2.2% of the time in babies that weigh less than 8 pounds 13 ounces (4,000 g), 13.9% of the time in babies that weigh 8 pounds 13 ounces (4,000 g) to 9 pounds 15 ounces (4,500 g), and 52.5% of the time in babies that weigh more than 9 pounds 15 ounces (4,500 g). [11] Although big babies are at higher risk for shoulder dystocia, most cases of shoulder dystocia happen in smaller babies because there are many more small and normal-size babies being born than big babies. [12] Researchers have been unable to predict who will have shoulder dystocia and who will not. [13] LGA babies are at higher risk of hypoglycemia in the neonatal period, independent of whether the mother has diabetes. [14] Hypoglycemia, as well as hyperbilirubinemia and polycythemia, occur as a result of hyperinsulinemia in the fetus. [15] High birth weight may impact the baby in the long term. Macrosomic neonates are at a higher risk of being overweight and obese than their normal-weight counterparts later in life. [4] [16] Studies have shown that the long-term overweight risk is doubled when the birth weight is greater than 4,000 g. [17] The risk of having type 2 diabetes mellitus in adult life is 19% higher among macrosomic babies with birth weights heavier than 4,500 g compared to those with birth weights between 4,000 g and 4,500 g. [18] Maternal [ edit ] Maternal complications in pregnancies with macrosomia include emergency cesarean section, postpartum hemorrhage and obstetric anal sphincter injury. [19] The risk of maternal complications in pregnancies with newborns weighing between 4,000 g and 4,500 g is two-fold greater than in pregnancies without macrosomia. ... The Journal of Pediatrics . 140 (2): 200–4. doi : 10.1067/mpd.2002.121696 . PMID 11865271 . ^ a b c d e f g h Boulvain M, Irion O, Dowswell T, Thornton JG, et al. ... PMID 30486715 . ^ a b Beta J, Khan N, Khalil A, Fiolna M, Ramadan G, Akolekar R (September 2019). "Maternal and neonatal complications of fetal macrosomia: systematic review and meta-analysis" . ... PMID 19609940 . ^ Boubred F, Pauly V, Romain F, Fond G, Boyer L (2020-06-05). Farrar D (ed.).

-
Glutaric Acidemia Type 2
Wikipedia
Retrieved 30 August 2018 . ^ a b c d e f g "Glutaric acidemia type II" . Genetic and Rare Diseases Information Center (GARD) . ... National Library of Medicine External links [ edit ] Classification D ICD - 10 : E72.3 ICD - 9-CM : 277.85 OMIM : 231680 MeSH : D054069 DiseasesDB : 29816 v t e Inborn error of amino acid metabolism K → acetyl-CoA Lysine /straight chain Glutaric acidemia type 1 type 2 Hyperlysinemia Pipecolic acidemia Saccharopinuria Leucine 3-hydroxy-3-methylglutaryl-CoA lyase deficiency 3-Methylcrotonyl-CoA carboxylase deficiency 3-Methylglutaconic aciduria 1 Isovaleric acidemia Maple syrup urine disease Tryptophan Hypertryptophanemia G G→ pyruvate → citrate Glycine D-Glyceric acidemia Glutathione synthetase deficiency Sarcosinemia Glycine → Creatine : GAMT deficiency Glycine encephalopathy G→ glutamate → α-ketoglutarate Histidine Carnosinemia Histidinemia Urocanic aciduria Proline Hyperprolinemia Prolidase deficiency Glutamate / glutamine SSADHD G→ propionyl-CoA → succinyl-CoA Valine Hypervalinemia Isobutyryl-CoA dehydrogenase deficiency Maple syrup urine disease Isoleucine 2-Methylbutyryl-CoA dehydrogenase deficiency Beta-ketothiolase deficiency Maple syrup urine disease Methionine Cystathioninuria Homocystinuria Hypermethioninemia General BC / OA Methylmalonic acidemia Methylmalonyl-CoA mutase deficiency Propionic acidemia G→ fumarate Phenylalanine / tyrosine Phenylketonuria 6-Pyruvoyltetrahydropterin synthase deficiency Tetrahydrobiopterin deficiency Tyrosinemia Alkaptonuria / Ochronosis Tyrosinemia type I Tyrosinemia type II Tyrosinemia type III / Hawkinsinuria Tyrosine → Melanin Albinism : Ocular albinism ( 1 ) Oculocutaneous albinism ( Hermansky–Pudlak syndrome ) Waardenburg syndrome Tyrosine → Norepinephrine Dopamine beta hydroxylase deficiency reverse: Brunner syndrome G→ oxaloacetate Urea cycle / Hyperammonemia ( arginine aspartate ) Argininemia Argininosuccinic aciduria Carbamoyl phosphate synthetase I deficiency Citrullinemia N-Acetylglutamate synthase deficiency Ornithine transcarbamylase deficiency / translocase deficiency Transport / IE of RTT Solute carrier family : Cystinuria Hartnup disease Iminoglycinuria Lysinuric protein intolerance Fanconi syndrome : Oculocerebrorenal syndrome Cystinosis Other 2-Hydroxyglutaric aciduria Aminoacylase 1 deficiency Ethylmalonic encephalopathy Fumarase deficiency Trimethylaminuria v t e Inborn error of lipid metabolism : fatty-acid metabolism disorders Synthesis Biotinidase deficiency (BTD) Degradation Acyl transport Carnitine CPT1 CPT2 CDSP CACTD Adrenoleukodystrophy (ALD) Beta oxidation General Acyl CoA dehydrogenase Short-chain SCADD Medium-chain MCADD Long-chain 3-hydroxy LCHAD Very long-chain VLCADD Mitochondrial trifunctional protein deficiency (MTPD): Acute fatty liver of pregnancy Unsaturated 2,4 Dienoyl-CoA reductase deficiency (DECRD) Odd chain Propionic acidemia (PCC deficiency) Other 3-hydroxyacyl-coenzyme A dehydrogenase deficiency (HADHD) Glutaric acidemia type 2 (MADD) To acetyl-CoA Malonic aciduria (MCD) Aldehyde Sjögren–Larsson syndrome (SLS)
-
Hyperammonemia
Wikipedia
.; Capocaccia, L.; Caschera, M.; Zullo, A.; Pinto, G.; Gaudio, E.; Franchitto, A.; Spagnoli, R.; D'Aquilino, E. ... External links [ edit ] Classification D ICD - 10 : E72.2 ICD - 9-CM : 270.6 MeSH : D022124 DiseasesDB : 20468 External resources eMedicine : neuro/162 ped/1057 v t e Inborn error of amino acid metabolism K → acetyl-CoA Lysine /straight chain Glutaric acidemia type 1 type 2 Hyperlysinemia Pipecolic acidemia Saccharopinuria Leucine 3-hydroxy-3-methylglutaryl-CoA lyase deficiency 3-Methylcrotonyl-CoA carboxylase deficiency 3-Methylglutaconic aciduria 1 Isovaleric acidemia Maple syrup urine disease Tryptophan Hypertryptophanemia G G→ pyruvate → citrate Glycine D-Glyceric acidemia Glutathione synthetase deficiency Sarcosinemia Glycine → Creatine : GAMT deficiency Glycine encephalopathy G→ glutamate → α-ketoglutarate Histidine Carnosinemia Histidinemia Urocanic aciduria Proline Hyperprolinemia Prolidase deficiency Glutamate / glutamine SSADHD G→ propionyl-CoA → succinyl-CoA Valine Hypervalinemia Isobutyryl-CoA dehydrogenase deficiency Maple syrup urine disease Isoleucine 2-Methylbutyryl-CoA dehydrogenase deficiency Beta-ketothiolase deficiency Maple syrup urine disease Methionine Cystathioninuria Homocystinuria Hypermethioninemia General BC / OA Methylmalonic acidemia Methylmalonyl-CoA mutase deficiency Propionic acidemia G→ fumarate Phenylalanine / tyrosine Phenylketonuria 6-Pyruvoyltetrahydropterin synthase deficiency Tetrahydrobiopterin deficiency Tyrosinemia Alkaptonuria / Ochronosis Tyrosinemia type I Tyrosinemia type II Tyrosinemia type III / Hawkinsinuria Tyrosine → Melanin Albinism : Ocular albinism ( 1 ) Oculocutaneous albinism ( Hermansky–Pudlak syndrome ) Waardenburg syndrome Tyrosine → Norepinephrine Dopamine beta hydroxylase deficiency reverse: Brunner syndrome G→ oxaloacetate Urea cycle / Hyperammonemia ( arginine aspartate ) Argininemia Argininosuccinic aciduria Carbamoyl phosphate synthetase I deficiency Citrullinemia N-Acetylglutamate synthase deficiency Ornithine transcarbamylase deficiency / translocase deficiency Transport / IE of RTT Solute carrier family : Cystinuria Hartnup disease Iminoglycinuria Lysinuric protein intolerance Fanconi syndrome : Oculocerebrorenal syndrome Cystinosis Other 2-Hydroxyglutaric aciduria Aminoacylase 1 deficiency Ethylmalonic encephalopathy Fumarase deficiency TrimethylaminuriaNAGS, CPS1, OTC, GLUD1, ASS1, TLR5, TYMS, GOT2, PRKCQ, GLUL, ARG1, ASL, SLC25A15, SLC25A13, HMGCL, HADH, MMUT, NR1H4, TMEM70, CA5A, ATP5F1D, ACAD9, NDUFA6, MMAA, HLCS, TANGO2, IVD, ATPAF2, SERAC1, ACADM, PCCA, MCCC2, NBAS, PCCB, MCCC1, SLC22A5, TUFM, UQCRC2, SLC7A7, HADHA, HADHB, ACADL, MMAB, ACADVL, ACAT1, BTD, SLC25A20, CAD, CPT1A, CPT2, CYC1, DLD, GCK, MSTN, TFEB, CTNNB1, TNF, GRIA2, GRIA1, HNF4A, OAT, PC, IL1B, CRK, INSR, AHSA1, RNF19A, POLDIP2, CAT, ATP6V0A4, MED18, MAPK14, IL1A, TWNK, BDNF, ARG2, AMT, ALB, GSK3B, GRAP2, AIMP2, GCSH, SLC6A6, OGDH, PCNA, ABCB1, POLG, GABPA, MAPK1, ROS1, CCL4, SLC9A1, GLS, ABCC8, CYP2C9, GSR, TNFRSF1A, TNFRSF1B, CYP2A6, NFE2L2, GFAP, HSD17B10

-
Diabetes And Deafness, Maternally Inherited
OMIM
The most common mutation is a 3243A-G transition in the MTTL1 gene (590050.0001). ... Velho et al. (1996) reported 5 French pedigrees with the common 3243A-G mutation associated with variable clinical features, ranging from normal glucose tolerance to insulin-requiring diabetes. ... Reardon et al. (1992) identified the 3243A-G mutation in the MTTL1 gene in a family with MIDD. ... Since the level of mutated mtDNA in hair follicles was most similar to the level in muscle, the authors suggested that hair follicles may be the best tissue for noninvasive quantitation of the 3243A-G mutation. Sue et al. (1993) and Schulz et al. (1993) identified the 3243A-G mutation in affected individuals. ... Mutation in the MTTK Gene Kameoka et al. (1998) identified an 8396A-G mutation in the MTTK gene (590060.0005) in patients with maternally inherited diabetes and deafness.

-
Retrocolic Hernia
Wikipedia
It has been observed to occur as a complication of a left hemicolectomy . [1] References [ edit ] ^ Angelone, G; Giardiello, C; Francica, G (October 2005).
-
Fibrinogenolysis
Wikipedia
"Consumptive thrombohemorrhagic disorders". Hematology . ^ Potron G, Caen JP, Tobelem G, Soria C, eds. (1988).
-
Erythrocyanosis Crurum
Wikipedia
See also [ edit ] Chilblains List of cutaneous conditions References [ edit ] Otto Braun-Falco; G. Plewig; H. H. Wolff; Walter H. C. ... James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: Clinical Dermatology .
-
Childhood Granulomatous Periorificial Dermatitis
Wikipedia
After CGPD resolves, the skin may return to normal without scarring or may have small atrophic depressions with collagen loss , milia , or small pit-like scars. [1] Epidemiology [ edit ] CGPD occurs most often in children of Afro-Caribbean descent before puberty though reports of this disease occurring in Asian and Caucasian children have also been described. [1] [3] Due to the limited number of reported cases, it remains controversial whether CGPD occurs more often in African children than in children of other races. [2] CGPD is more common in boys than girls. [3] History [ edit ] Gianotti et al. first described CGPD in five Italian children in 1970. [3] In 1990, Williams et al. described a similar skin eruption in five children of Afro-Caribbean descent and coined the proposed term "facial Afro-Caribbean childhood eruption (FACE)". [3] Subsequently, another article by Katz and Lesher first introduced the term CGPD since some reported cases were not found in children of Afro-Caribbean descent and to avoid confusion with perioral dermatitis. [3] See also [ edit ] Perioral dermatitis References [ edit ] ^ a b c d e f g h i j k l m Dessinioti, C; Antoniou, C; Katsambas, A (January–February 2014). ... Clinics in Dermatology (Review). 32 (1): 24–34. doi : 10.1016/j.clindermatol.2013.05.023 . PMID 24314375 . ^ a b c d e f g h i j Zalaudek, I; Di Stefani, A; Ferrara, G; Argenziano, G (April 2005). ... PMID 16370472 . S2CID 9802651 . ^ a b c d e f g h i Kim, YJ; Shin, JW; Lee, JS; Park, YL; Whang, KU; Lee, SY (August 2011).
-
Musk, Inability To Smell
OMIM
The guanine nucleotide-binding proteins (G or N proteins) are ubiquitous features of signal transduction mechanisms involving control of intracellular calcium and second messengers, regulation of cell growth, gating of ion channels, olfaction, vision, and possibly other sensory systems. Possibly because of their key role in signal transduction, G proteins have been singled out as targets by toxins from several types of bacteria, e.g., those causing diphtheria, cholera, and pertussis. These toxins have proved valuable in identifying the function of the different G proteins (Dolphin, 1987). It is possible that specific anosmia or 'smell blindness' in the olfactory system is analogous to colorblindness in vision, where unequal crossing over between the highly homologous receptors within a cluster during gametogenesis results in the formation of new hybrid receptors and/or the deletion of receptor genes (Reed, 1996).
-
Acquired Idiopathic Generalized Anhidrosis
Wikipedia
However, these refined methods are mostly used for research purposes and not generally available. [5] Skin biopsy analysis may play a crucial role in the identification of AIGA subgroups. [1] See also [ edit ] Hypohidrosis References [ edit ] ^ a b Chen, Y. C.; Wu, C. S.; Chen, G. S.; Khor, G. T.; Chen, C. H.; Huang, P. (2008). ... PMID 15505168 . ^ Donadio, V.; Montagna, P.; Nolano, M.; Cortelli, P.; Misciali, C.; Pierangeli, G.; Provitera, V.; Casano, A.; Baruzzi, A.; Liguori, R. (2005).
-
Abdominal Compartment Syndrome
Wikipedia
J.; De laet, I.; Malbrain, M. L. N. G. (12 October 2015). "Understanding abdominal compartment syndrome". ... PMID 23673399 . ^ Malbrain, Manu L. N. G.; Cheatham, Michael L.; Kirkpatrick, Andrew; Sugrue, Michael; Parr, Michael; De Waele, Jan; Balogh, Zsolt; Leppäniemi, Ari; Olvera, Claudia (2006-11-01). ... PMID 19186280 . ^ van Brunschot, Sandra; Schut, Anne Julia; Bouwense, Stefan A.; Besselink, Marc G.; Bakker, Olaf J.; van Goor, Harry; Hofker, Sijbrand; Gooszen, Hein G.; Boermeester, Marja A.; van Santvoort, Hjalmar C. (2014). ... J.; De laet, I.; Malbrain, M. L. N. G. (12 October 2015). "Understanding abdominal compartment syndrome". ... S2CID 9692082 . ^ Patel, Aashish; Lall, Chandana G.; Jennings, S. Gregory; Sandrasegaran, Kumaresan (November 2007).
-
Olive Quick Decline Syndrome
Wikipedia
. ^ Saponari, M.; Boscia, D.; Altamura, G.; Loconsole, G.; Zicca, S.; D’Attoma, G.; Morelli, M.; Palmisano, F.; Saponari, A.; Tavano, D.; Savino, V. ... PMC 5735170 . PMID 29255232 . ^ Martelli, G. P.; Boscia, D.; Porcelli, F.; Saponari, M. (1 February 2016).

-
Aggressive Angiomyxoma
Wikipedia
. ^ Mathieson A, Chandrakanth S, Yousef G, Wadden P (June 2007). "Aggressive angiomyxoma of the pelvis: a case report" (PDF) . ... PMID 18295664 . ^ Medeiros, F; Erickson-Johnson, M. R.; Keeney, G. L.; Clayton, A. C.; Nascimento, A. G.; Wang, X; Oliveira, A. M. (2007). ... R.; Weremowicz, S; Neskey, D. M.; Sornberger, K; Tallini, G; Morton, C. C.; Quade, B. J. (2001). ... R.; Weremowicz, S; Neskey, D. M.; Sornberger, K; Tallini, G; Morton, C. C.; Quade, B. J. (2001).

-
Citrullinemia
Wikipedia
National Library of Medicine External links [ edit ] Classification D ICD - 10 : E72.2 ICD - 9-CM : 270.6 OMIM : 215700 605814 603471 MeSH : D020159 DiseasesDB : 29676 External resources eMedicine : ped/406 v t e Inborn error of amino acid metabolism K → acetyl-CoA Lysine /straight chain Glutaric acidemia type 1 type 2 Hyperlysinemia Pipecolic acidemia Saccharopinuria Leucine 3-hydroxy-3-methylglutaryl-CoA lyase deficiency 3-Methylcrotonyl-CoA carboxylase deficiency 3-Methylglutaconic aciduria 1 Isovaleric acidemia Maple syrup urine disease Tryptophan Hypertryptophanemia G G→ pyruvate → citrate Glycine D-Glyceric acidemia Glutathione synthetase deficiency Sarcosinemia Glycine → Creatine : GAMT deficiency Glycine encephalopathy G→ glutamate → α-ketoglutarate Histidine Carnosinemia Histidinemia Urocanic aciduria Proline Hyperprolinemia Prolidase deficiency Glutamate / glutamine SSADHD G→ propionyl-CoA → succinyl-CoA Valine Hypervalinemia Isobutyryl-CoA dehydrogenase deficiency Maple syrup urine disease Isoleucine 2-Methylbutyryl-CoA dehydrogenase deficiency Beta-ketothiolase deficiency Maple syrup urine disease Methionine Cystathioninuria Homocystinuria Hypermethioninemia General BC / OA Methylmalonic acidemia Methylmalonyl-CoA mutase deficiency Propionic acidemia G→ fumarate Phenylalanine / tyrosine Phenylketonuria 6-Pyruvoyltetrahydropterin synthase deficiency Tetrahydrobiopterin deficiency Tyrosinemia Alkaptonuria / Ochronosis Tyrosinemia type I Tyrosinemia type II Tyrosinemia type III / Hawkinsinuria Tyrosine → Melanin Albinism : Ocular albinism ( 1 ) Oculocutaneous albinism ( Hermansky–Pudlak syndrome ) Waardenburg syndrome Tyrosine → Norepinephrine Dopamine beta hydroxylase deficiency reverse: Brunner syndrome G→ oxaloacetate Urea cycle / Hyperammonemia ( arginine aspartate ) Argininemia Argininosuccinic aciduria Carbamoyl phosphate synthetase I deficiency Citrullinemia N-Acetylglutamate synthase deficiency Ornithine transcarbamylase deficiency / translocase deficiency Transport / IE of RTT Solute carrier family : Cystinuria Hartnup disease Iminoglycinuria Lysinuric protein intolerance Fanconi syndrome : Oculocerebrorenal syndrome Cystinosis Other 2-Hydroxyglutaric aciduria Aminoacylase 1 deficiency Ethylmalonic encephalopathy Fumarase deficiency Trimethylaminuria

-
Smouldering Myeloma
Wikipedia
It is characterised as a pre-malignant disease that lacks symptoms but is associated with bone marrow biopsy showing the presence of an abnormal number of clonal myeloma cells, blood and/or urine containing a myeloma protein, and a significant risk of developing into a malignant disease. [2] Contents 1 Diagnosis 2 Treatment 3 Prognosis 4 References 5 Further reading Diagnosis [ edit ] Smouldering myeloma is characterised by: [4] Serum paraprotein >30 g/l or urinary monoclonal protein ≥500 mg per 24 h AND/OR Clonal plasma cells >10% and <60% on bone marrow biopsy AND No evidence of end organ damage that can be attributed to plasma cell disorder AND No myeloma-defining event (>60% plasma cells in bone marrow OR Involved/Uninvolved light chain ratio >100) Treatment [ edit ] Treatment for multiple myeloma is focused on therapies that decrease the clonal plasma cell population and consequently decrease the signs and symptoms of disease. ... PMID 24658815 . ^ Rajkumar, SV; Dimopoulos, MA; Palumbo, A; Blade, J; Merlini, G; Mateos, MV; Kumar, S; Hillengass, J; Kastritis, E; Richardson, P; Landgren, O; Paiva, B; Dispenzieri, A; Weiss, B; LeLeu, X; Zweegman, S; Lonial, S; Rosinol, L; Zamagni, E; Jagannath, S; Sezer, O; Kristinsson, SY; Caers, J; Usmani, SZ; Lahuerta, JJ; Johnsen, HE; Beksac, M; Cavo, M; Goldschmidt, H; Terpos, E; Kyle, RA; Anderson, KC; Durie, BG; Miguel, JF (November 2014). ... Further reading [ edit ] Barlogie B, van Rhee F, Shaughnessy JD, Epstein J, Yaccoby S, Pineda-Roman M, Hollmig K, Alsayed Y, Hoering A, Szymonifka J, Anaissie E, Petty N, Kumar NS, Srivastava G, Jenkins B, Crowley J, Zeldis JB (Oct 15, 2008). ... Pérez-Persona E, Vidriales MB, Mateo G, García-Sanz R, Mateos MV, de Coca AG, Galende J, Martín-Nuñez G, Alonso JM, de Las Heras N, Hernández JM, Martín A, López-Berges C, Orfao A, San Miguel JF (Oct 1, 2007). ... Kyle RA, Durie BG, Rajkumar SV, Landgren O, Blade J, Merlini G, Kröger N, Einsele H, Vesole DH, Dimopoulos M, San Miguel J, Avet-Loiseau H, Hajek R, Chen WM, Anderson KC, Ludwig H, Sonneveld P, Pavlovsky S, Palumbo A, Richardson PG, Barlogie B, Greipp P, Vescio R, Turesson I, Westin J, Boccadoro M (Jun 2010).






