-
Gerstmann-Straussler Disease
Omim
Arata et al. (2006) concluded that the sites of pathology in this group of patients were in the cerebrum and spinal cord, including the posterior horn and spinocerebellar tracts, instead of the cerebellum proper. ... Ghetti et al. (1996) noted that abnormal PRNP truncation at a similar site (between residues 144 and 150) occurs in GSS variants in which the amyloid protein has been analyzed, suggesting that this truncated PrP peptide is important for amyloid formation. ... Ghetti et al. (1996) noted that abnormal PRNP truncation at a similar site (between residues 144 and 150) occurs in GSS variants in which the amyloid protein has been analyzed, suggesting that this truncated PrP peptide is important for amyloid formation. ... INHERITANCE - Autosomal dominant GROWTH Weight - Rapid weight loss late in the disease HEAD & NECK Eyes - Impaired smooth pursuit NEUROLOGIC Central Nervous System - Cerebellar ataxia - Gait ataxia - Truncal ataxia - Limb ataxia - Lower limb weakness - Dysarthria - Memory loss - Dementia (later onset) - Extrapyramidal signs (less common) - Parkinsonism - Rigidity - Bradykinesia - Tremor - Apraxia - Spasticity - Hyperreflexia - Myoclonus - Perseveration - Amyloid-like plaques, immunoreactive to PrP, predominantly in the cerebellum - Amyloid-like plaques are not immunoreactive to APP ( 104760 ) - PRNP-immunoreactive cerebral amyloid angiopathy (in some patients) - Neurofibrillary tangles may be present - Spongiform changes are mild or may not be present - Some patients have periodic wave complexes on EEG - Cerebellar atrophy Peripheral Nervous System - Dysesthesias of the lower limbs - Loss of deep tendon reflexes Behavioral Psychiatric Manifestations - Personality changes - Aggressive behavior - Emotional lability - Depression - Psychosis MISCELLANEOUS - Adult onset, usually 30's to 40's, but up to early 60's - Rapidly progressive, but slower than Creutzfeldt-Jakob disease ( 123400 ) - Average disease duration of 7 years - Longer disease duration than Creutzfeldt-Jakob disease - Variable phenotype MOLECULAR BASIS - Caused by mutation in the prion protein gene (PRNP, 176640.0002 ) ▲ ClosePRNP, G6PC, C4BPA, PRDX2, ABCB6, CARD14, SLC37A4, PHKA2, APOE, SI, MGAM, APOB, TSHZ1, GCA, BTD, ABCG8, PYGM, CDHR5, NT5C3A, MED18, LINC01193, NCOA6, ECD, ABCG5, H3P36, TRAF3, H3C9P, HNF1A, POLDIP3, ROS1, SYNE1, ACHE, PYGL, PLCL1, ANXA2, APP, APRT, CCKAR, CSF3, CTLA4, CYP7A1, FABP2, GBE1, GH1, GNAS, GYG1, GYS2, IL6ST, LRPAP1, MAPT, MB, MDH1, MFAP1, MNAT1, ADRA2A, FAS-AS1
-
Paroxysmal Nocturnal Hemoglobinuria
Wikipedia
This is the main cause of severe complications and death in PNH. These may develop in common sites ( deep vein thrombosis of the leg and resultant pulmonary embolism when these clots break off and enter the lungs), but in PNH blood clots may also form in more unusual sites: the hepatic vein (causing Budd-Chiari syndrome ), the portal vein of the liver (causing portal vein thrombosis ), the superior or inferior mesenteric vein (causing mesenteric ischemia ) and veins of the skin. ... These include patients with unexplained thrombosis who are young, have thrombosis in an unusual site (e.g. intra-abdominal veins, cerebral veins, dermal veins), have any evidence of hemolysis (e.g. a raised LDH), or have a low red blood cell, white blood cell, or platelet count. [15] Those who have a diagnosis of aplastic anemia should be screened annually. [4] Treatment [ edit ] Acute attacks [ edit ] There is disagreement as to whether steroids (such as prednisolone ) can decrease the severity of hemolytic crises. ... ISBN 978-1-4160-2973-1 . ^ a b c d e f g h i j k l m n o p q r Parker C, Omine M, Richards S, et al. (2005). "Diagnosis and management of paroxysmal nocturnal hemoglobinuria" . ... PMID 23610373 . ^ Hall C, Richards S, Hillmen P (November 2003). "Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH)" . ... Dtsch Med Wochenschr (in German). 8 : 1–3 and 17–21. doi : 10.1055/s-0029-1196307 . ^ Marchiafava E, Nazari A (1911).PIGA, CD59, PIGT, CD34, FLNA, GPI, CD55, FCGR3B, CD14, TNF, FCGR3A, IFNG, BST1, HMGA2, CR1, IL10, KIR3DL1, PTPRC, CDR3, GEM, C3, CD48, CD24, HPRT1, RBM45, CFH, HLA-A, CSF2, HP, HLA-DRB1, ARFGEF2, IL6, SELL, KLRC4-KLRK1, FAS, PRTN3, FUT4, RN7SL263P, CSF3, CEACAM8, NEDD4L, KLRK1, SORBS1, CCL2, ERGIC2, TFRC, PGAP1, TFPI, TBCE, CRLS1, THPO, RPS6KA3, RPL6, POLR3E, PRNP, PMS1, PLG, PLAUR, PLAU, THBD, THY1, CAP1, CTC1, PIGF, ECI2, PIGM, EFS, NR1H4, HACD1, ADAMTS13, NOL3, BRD4, UBL4A, CD160, CBLL2, CLYBL, CXCR4, WT1, CCR2, MUL1, ACTB, SERPINB6, DAB1, G6PD, FUT1, FLT3LG, FES, FCGR1A, F2, EPO, EGR1, CELSR3, CFD, CTAA1, GYPA, ATF2, CD52, CD40, CD38, CD36, CD1D, C6, C5, BMPR2, SERPINC1, CBLIF, GYPB, ATP8B1, CXCL10, PRKN, NRAS, NFE2L2, MPO, MME, LNPEP, KIR3DL2, KIR2DS1, JAK2, AKT1, CXCR2, GYPE, IL2, IL1B, RBPJ, IGF1, IFNA13, IFNA1, IDH1, HTC2, HLA-DQA1, HLA-C, ITGB2

-
Hermansky–pudlak Syndrome
Wikipedia
The RLDC is dedicated to developing new diagnostics and therapeutics for patients with rare lung diseases, through collaboration between the NIH, patient organizations and clinical investigators. [ citation needed ] Society [ edit ] Hermansky–Pudlak syndrome patients, families, and caregivers are encouraged to join the NIH Rare Lung Diseases Consortium Contact Registry . This is a privacy protected site that provides up-to-date information for individuals interested in the latest scientific news, trials, and treatments related to rare lung diseases. [ citation needed ] Eponym [ edit ] It is named for František Heřmanský (1916–1980) and Pavel Pudlák (1927–1993). [14] [15] [16] See also [ edit ] Biogenesis of lysosome-related organelles complex 1 List of cutaneous conditions References [ edit ] ^ Oh, J; Ho, L; Ala-Mello, S; Amato, D; Armstrong, L; Bellucci, S; Carakushansky, G; Ellis, Jp; Fong, Ct; Green, Js; Heon, E; Legius, E; Levin, Av; Nieuwenhuis, Hk; Pinckers, A; Tamura, N; Whiteford, Ml; Yamasaki, H; Spritz, Ra (March 1998). ... External links [ edit ] GeneReviews/NCBI/NIH/UW entry on Hermansky-Pudlak Syndrome Classification D ICD - 10 : E70.3 ( ILDS E70.360) ICD - 10-CM : E70.331 ICD - 9-CM : 270.2 OMIM : 203300 MeSH : D022861 DiseasesDB : 29161 SNOMED CT : 9311003 External resources eMedicine : oph/713 derm/925 GeneReviews : Hermansky-Pudlak Syndrome Orphanet : 79430 v t e Inborn error of amino acid metabolism K → acetyl-CoA Lysine /straight chain Glutaric acidemia type 1 type 2 Hyperlysinemia Pipecolic acidemia Saccharopinuria Leucine 3-hydroxy-3-methylglutaryl-CoA lyase deficiency 3-Methylcrotonyl-CoA carboxylase deficiency 3-Methylglutaconic aciduria 1 Isovaleric acidemia Maple syrup urine disease Tryptophan Hypertryptophanemia G G→ pyruvate → citrate Glycine D-Glyceric acidemia Glutathione synthetase deficiency Sarcosinemia Glycine → Creatine : GAMT deficiency Glycine encephalopathy G→ glutamate → α-ketoglutarate Histidine Carnosinemia Histidinemia Urocanic aciduria Proline Hyperprolinemia Prolidase deficiency Glutamate / glutamine SSADHD G→ propionyl-CoA → succinyl-CoA Valine Hypervalinemia Isobutyryl-CoA dehydrogenase deficiency Maple syrup urine disease Isoleucine 2-Methylbutyryl-CoA dehydrogenase deficiency Beta-ketothiolase deficiency Maple syrup urine disease Methionine Cystathioninuria Homocystinuria Hypermethioninemia General BC / OA Methylmalonic acidemia Methylmalonyl-CoA mutase deficiency Propionic acidemia G→ fumarate Phenylalanine / tyrosine Phenylketonuria 6-Pyruvoyltetrahydropterin synthase deficiency Tetrahydrobiopterin deficiency Tyrosinemia Alkaptonuria / Ochronosis Tyrosinemia type I Tyrosinemia type II Tyrosinemia type III / Hawkinsinuria Tyrosine → Melanin Albinism : Ocular albinism ( 1 ) Oculocutaneous albinism ( Hermansky–Pudlak syndrome ) Waardenburg syndrome Tyrosine → Norepinephrine Dopamine beta hydroxylase deficiency reverse: Brunner syndrome G→ oxaloacetate Urea cycle / Hyperammonemia ( arginine aspartate ) Argininemia Argininosuccinic aciduria Carbamoyl phosphate synthetase I deficiency Citrullinemia N-Acetylglutamate synthase deficiency Ornithine transcarbamylase deficiency / translocase deficiency Transport / IE of RTT Solute carrier family : Cystinuria Hartnup disease Iminoglycinuria Lysinuric protein intolerance Fanconi syndrome : Oculocerebrorenal syndrome Cystinosis Other 2-Hydroxyglutaric aciduria Aminoacylase 1 deficiency Ethylmalonic encephalopathy Fumarase deficiency Trimethylaminuria v t e Disorders of bleeding and clotting Coagulation · coagulopathy · Bleeding diathesis Clotting By cause Clotting factors Antithrombin III deficiency Protein C deficiency Activated protein C resistance Protein S deficiency Factor V Leiden Prothrombin G20210A Platelets Sticky platelet syndrome Thrombocytosis Essential thrombocythemia DIC Purpura fulminans Antiphospholipid syndrome Clots Thrombophilia Thrombus Thrombosis Virchow's triad Trousseau sign of malignancy By site Deep vein thrombosis Bancroft's sign Homans sign Lisker's sign Louvel's sign Lowenberg's sign Peabody's sign Pratt's sign Rose's sign Pulmonary embolism Renal vein thrombosis Bleeding By cause Thrombocytopenia Thrombocytopenic purpura : ITP Evans syndrome TM TTP Upshaw–Schulman syndrome Heparin-induced thrombocytopenia May–Hegglin anomaly Platelet function adhesion Bernard–Soulier syndrome aggregation Glanzmann's thrombasthenia platelet storage pool deficiency Hermansky–Pudlak syndrome Gray platelet syndrome Clotting factor Hemophilia A/VIII B/IX C/XI von Willebrand disease Hypoprothrombinemia/II Factor VII deficiency Factor X deficiency Factor XII deficiency Factor XIII deficiency Dysfibrinogenemia Congenital afibrinogenemia Signs and symptoms Bleeding Bruise Hematoma Petechia Purpura Nonthrombocytopenic purpura By site head Epistaxis Hemoptysis Intracranial hemorrhage Hyphema Subconjunctival hemorrhage torso Hemothorax Hemopericardium Pulmonary hematoma abdomen Gastrointestinal bleeding Hemobilia Hemoperitoneum Hematocele Hematosalpinx joint Hemarthrosis v t e Pigmentation disorders / Dyschromia Hypo- / leucism Loss of melanocytes Vitiligo Quadrichrome vitiligo Vitiligo ponctué Syndromic Alezzandrini syndrome Vogt–Koyanagi–Harada syndrome Melanocyte development Piebaldism Waardenburg syndrome Tietz syndrome Loss of melanin / amelanism Albinism Oculocutaneous albinism Ocular albinism Melanosome transfer Hermansky–Pudlak syndrome Chédiak–Higashi syndrome Griscelli syndrome Elejalde syndrome Griscelli syndrome type 2 Griscelli syndrome type 3 Other Cross syndrome ABCD syndrome Albinism–deafness syndrome Idiopathic guttate hypomelanosis Phylloid hypomelanosis Progressive macular hypomelanosis Leukoderma w/o hypomelanosis Vasospastic macule Woronoff's ring Nevus anemicus Ungrouped Nevus depigmentosus Postinflammatory hypopigmentation Pityriasis alba Vagabond's leukomelanoderma Yemenite deaf-blind hypopigmentation syndrome Wende–Bauckus syndrome Hyper- Melanin / Melanosis / Melanism Reticulated Dermatopathia pigmentosa reticularis Pigmentatio reticularis faciei et colli Reticulate acropigmentation of Kitamura Reticular pigmented anomaly of the flexures Naegeli–Franceschetti–Jadassohn syndrome Dyskeratosis congenita X-linked reticulate pigmentary disorder Galli–Galli disease Revesz syndrome Diffuse/ circumscribed Lentigo / Lentiginosis : Lentigo simplex Liver spot Centrofacial lentiginosis Generalized lentiginosis Inherited patterned lentiginosis in black persons Ink spot lentigo Lentigo maligna Mucosal lentigines Partial unilateral lentiginosis PUVA lentigines Melasma Erythema dyschromicum perstans Lichen planus pigmentosus Café au lait spot Poikiloderma ( Poikiloderma of Civatte Poikiloderma vasculare atrophicans ) Riehl melanosis Linear Incontinentia pigmenti Scratch dermatitis Shiitake mushroom dermatitis Other/ ungrouped Acanthosis nigricans Freckle Familial progressive hyperpigmentation Pallister–Killian syndrome Periorbital hyperpigmentation Photoleukomelanodermatitis of Kobori Postinflammatory hyperpigmentation Transient neonatal pustular melanosis Other pigments Iron Hemochromatosis Iron metallic discoloration Pigmented purpuric dermatosis Schamberg disease Majocchi's disease Gougerot–Blum syndrome Doucas and Kapetanakis pigmented purpura / Eczematid-like purpura of Doucas and Kapetanakis Lichen aureus Angioma serpiginosum Hemosiderin hyperpigmentation Other metals Argyria Chrysiasis Arsenic poisoning Lead poisoning Titanium metallic discoloration Other Carotenosis Tar melanosis Dyschromia Dyschromatosis symmetrica hereditaria Dyschromatosis universalis hereditaria See also Skin color Skin whitening Tanning Sunless Tattoo removal Depigmentation v t e Inherited disorders of trafficking / vesicular transport proteins Vesicle formation Lysosome / Melanosome : HPS1 – HPS7 Hermansky–Pudlak syndrome LYST Chédiak–Higashi syndrome COPII : SEC23A Cranio-lenticulo-sutural dysplasia COG7 CDOG IIE APC: AP1S2 X-linked intellectual disability AP3B1 Hermansky–Pudlak syndrome 2 AP4M1 CPSQ3 Rab ARL6 BBS3 RAB27A Griscelli syndrome 2 CHM Choroideremia MLPH Griscelli syndrome 3 Cytoskeleton Myosin : MYO5A Griscelli syndrome 1 Microtubule : SPG4 Hereditary spastic paraplegia 4 Kinesin : KIF5A Hereditary spastic paraplegia 10 Spectrin : SPTBN2 Spinocerebellar ataxia 5 Vesicle fusion Synaptic vesicle : SNAP29 CEDNIK syndrome STX11 Hemophagocytic lymphohistiocytosis 4 Caveolae : CAV1 Congenital generalized lipodystrophy 3 CAV3 Limb-girdle muscular dystrophy 2B , Long QT syndrome 9 Vacuolar protein sorting : VPS33B ARC syndrome VPS13B Cohen syndrome DYSF Distal muscular dystrophy See also vesicular transport proteinsHPS4, HPS3, BLOC1S3, DTNBP1, BLOC1S6, HPS6, HPS5, AP3D1, AP3B1, HPS1, RAB38, BLOC1S4, BLOC1S5, VPS33A, SLC7A11, KXD1, RABGGTA, CP, TFF1, MARK4, FGL1, TYRP1, RAB32, CD63, TYR, PI4K2A, RASGRF1, SOS1, OCA2, LGALS3, CHI3L1, SLC2A4RG, PDIA2, FUZ, FBXW7, MAP1LC3B, PADI1, BHLHE22, SLC35D3, PRDX5, PWAR4, VPS39, ACTB, HSPB3, NXF1, ABCC4, CD1B, CHM, LYST, ELANE, F2R, GDI1, HLA-C, P2RY1, P4HB, PAWR, PAX6, RMRP, SFTPC, PMEL, TNF, VWF, TCAP, VAMP8, SLC25A20, F2RL3, ARHGEF2, RAB9A, RIMS2, SFTPA1

-
Growth Hormone Deficiency
Wikipedia
Nearly painless insulin syringes , pen injectors , or a needle-free delivery system reduce the discomfort. Injection sites include the biceps, thigh, buttocks, and stomach. Injection sites should be rotated daily to avoid lipoatrophy. ... Cost of adult treatment in the UK is 3000-4000 GBP annually. [16] Side effects [ edit ] Headaches Joint pain and muscle pain Fluid retention , and carpal tunnel syndrome Mild hypertension Visual problems Nausea and vomiting Paraesthesiae Antibody formation Reactions at the injection site Rarely, benign intracranial hypertension . [8] Prognosis [ edit ] Child [ edit ] When treated with GH, a severely deficient child will begin to grow faster within months. ... Metab . 87 (3): 1402–6. doi : 10.1210/jc.87.3.1402 . PMID 11889216 . ^ Saborio P, Hahn S, Hisano S, Latta K, Scheinman JI, Chan JC (October 1998). ... S2CID 46847002 . ^ a b Molitch ME, Clemmons DR, Malozowski S, et al. (May 2006). "Evaluation and treatment of adult growth hormone deficiency: an Endocrine Society Clinical Practice Guideline" .POU1F1, RNPC3, GHRHR, GHRH, GHSR, KISS1R, KISS1, CSHL1, NR5A1, GH1, TG, TACR3, GNRH1, GNRHR, HESX1, SOX3, LHX4, GLI2, PROP1, OTX2, LHX3, IGF1, GHR, IGHD, IGFBP3, SLC20A1, BTK, PHEX, PAX6, FBXO8, GPR101, HGH1, FBRS, ALB, SDS, SOAT1, SHBG, BRD2, PRL, MMUT, POMC
-
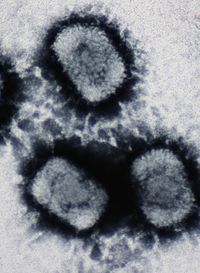
Cowpox
Wikipedia
The arm-to-arm method of transfer of the cowpox vaccine was also used to distribute Jenner's vaccine throughout the Spanish Empire. Spanish king Charles IV 's daughter had been stricken with smallpox in 1798, and after she recovered, he arranged for the rest of his family to be vaccinated. ... One way individuals expressed their discontent was to draw comics that sometimes depicted small cows growing from the sites of vaccination. Others publicly advocated for the continuance of the inoculations; however, this was not because of their discontent for the vaccinations. ... Symptoms of infection with cowpox virus in humans are localized, pustular lesions generally found on the hands and limited to the site of introduction. The incubation period is nine to ten days. ... ISBN 978-0-87113-830-9 . ^ Noyce RS, Lederman S, Evans DH (2018-01-19). Thiel V (ed.). ... ISBN 978-1-84222-150-1 . ^ Yuan, Jenifer The Small Pox Story ^ Riedel S (January 2005). "Edward Jenner and the history of smallpox and vaccination" .FLNB, SEC14L2, NXF1, USO1, TNF, XIAP, TAP1, SAMD9L, MTUS1, SAMD9, IL18, CASP1, CXCL8, IL1B, CXCL1, CDS1, CD86, CD80, STING1
-
Central Cord Syndrome
Wikipedia
It accounts for approximately 9% of traumatic SCIs. [4] After an incomplete injury, the brain still has the capacity to send and receive some signals below the site of injury. Sending and receiving of signals to and from parts of the body is reduced, not entirely blocked. ... PMID 13222164 . ^ a b c Harrop, James S; Ashwini Sharan; Jonathon Ratliff (2006). ... Physical Medicine and Rehabilitation Clinics of North America . 18 (2): 183–202. doi : 10.1016/j.pmr.2007.02.002 . PMID 17543768 . ^ Yadla, S.; Klimo, J.; Harrop, J.S. (2010). ... Topics in Spinal Cord Injury Rehabilitation . 15 (3): 73–84. doi : 10.1310/sci1503-73 . ^ Yadla, Sanjay; Paul Klimo; James S. Harrop (2010). "Traumatic Central Cord Syndrome: Etiology, Management, and Outcomes" .

-
Odontoma
Wikipedia
. ^ Junquera L, de Vicente JC, Roig P, Olay S, Rodríguez-Recio O (2005). "Intraosseous odontoma erupted into the oral cavity: an unusual pathology" (PDF) . ... Retrieved 2009-01-04 . ^ Bhargavan Sarojini S, Khosla E, Varghese T, Johnson Arakkal L (2014). ... PMC 4037568 . PMID 24900927 . ^ Amado Cuesta S, Gargallo Albiol J, Berini Aytés L, Gay Escoda C (2003). ... Retrieved 3 August 2019 . ^ Saavetha's Surgical and Pathological Excellence in Unmasking 256 Teeth from a Single Site in a Child , 1 August 2019 News from Saavetha Dental College , Chennai .

-
Vitamin K Deficiency Bleeding
Wikipedia
Vitamin K deficiency leads to the risk of blood coagulation problems due to impaired production of clotting factors II, VII, IX, X, protein C and protein S by the liver . More rarely VKDB can be caused by maternal medicines causing vitamin K deficiency in the newborn. [2] VKDB can largely be prevented by prophylactic supplementation of vitamin K, which is typically given shortly after birth by intramuscular injection. ... Contents 1 Classification 2 Signs and symptoms 3 Causes 4 Diagnosis 5 Prevention 5.1 Controversy 6 Treatment 7 References 8 External links Classification [ edit ] VKDB is classified as early, classical or late depending on when it first starts with each having somewhat different types of bleeding and underlying cause: Classification of vitamin K deficiency in the newborn (VKDB) [2] Syndrome Time of onset Common sites of bleeding Potential causes Early First 24 hours Scalp, skin, brain, chest, abdomen Maternal medications Classical 1-7 days Gut, umbilicus, skin, nose, circumcision Idiopathic , breast feeding Late After day 8 Brain, skin, gut Idiopathic, breast feeding, cholestasis Signs and symptoms [ edit ] VKDB presents typically in the first month of life with bleeding which can be from various locations. ... Thrombosis and Haemostasis . 81 (3): 456–461. doi : 10.1055/s-0037-1614494 . ^ a b c d e f g h i j k l m Shearer, Martin J. ... Pediatrics . 112 (1 Pt 1): 191–2. doi : 10.1542/peds.112.1.191 . PMID 12837888 . ^ Logan S, Gilbert R (1998). "Vitamin K For Newborn Babies" (PDF) .

-
Embryonal Carcinoma
Wikipedia
So in the testicle , they are often observed as blue cells attempting to form primitive tubules . [5] References [ edit ] ^ a b c d Mills, S (ed.) 2009. Sternberg's Diagnostic Pathology. 5th Edition. ... ISBN 978-81-312-1036-9 . ^ a b Kao, C. S.; Ulbright, T. M.; Young, R. H.; Idrees, M. ... MedicineNet.com. 26 October 2005 v t e Germ cell tumors Germinomatous Germinoma Seminoma Dysgerminoma Nongerminomatous Embryonal carcinoma Endodermal sinus tumor/Yolk sac tumor Teratoma : Fetus in fetu Dermoid cyst Struma ovarii Strumal carcinoid Trophoblastic neoplasm : Gestational trophoblastic disease Hydatidiform mole Choriocarcinoma Placental site trophoblastic tumor Polyembryoma Gonadoblastoma v t e Tumors of the female urogenital system Adnexa Ovaries Glandular and epithelial / surface epithelial- stromal tumor CMS: Ovarian serous cystadenoma Mucinous cystadenoma Cystadenocarcinoma Papillary serous cystadenocarcinoma Krukenberg tumor Endometrioid tumor Clear-cell ovarian carcinoma Brenner tumour Sex cord–gonadal stromal Leydig cell tumour Sertoli cell tumour Sertoli–Leydig cell tumour Thecoma Granulosa cell tumour Luteoma Sex cord tumour with annular tubules Germ cell Dysgerminoma Nongerminomatous Embryonal carcinoma Endodermal sinus tumor Gonadoblastoma Teratoma / Struma ovarii Choriocarcinoma Fibroma Meigs' syndrome Fallopian tube Adenomatoid tumor Uterus Myometrium Uterine fibroids/leiomyoma Leiomyosarcoma Adenomyoma Endometrium Endometrioid tumor Uterine papillary serous carcinoma Endometrial intraepithelial neoplasia Uterine clear-cell carcinoma Cervix Cervical intraepithelial neoplasia Clear-cell carcinoma SCC Glassy cell carcinoma Villoglandular adenocarcinoma Placenta Choriocarcinoma Gestational trophoblastic disease General Uterine sarcoma Mixed Müllerian tumor Vagina Squamous-cell carcinoma of the vagina Botryoid rhabdomyosarcoma Clear-cell adenocarcinoma of the vagina Vaginal intraepithelial neoplasia Vaginal cysts Vulva SCC Melanoma Papillary hidradenoma Extramammary Paget's disease Vulvar intraepithelial neoplasia Bartholin gland carcinoma v t e Tumors of the male urogenital system Testicles Sex cord– gonadal stromal Sertoli–Leydig cell tumour Sertoli cell tumour Leydig cell tumour Germ cell G Seminoma Spermatocytic tumor Germ cell neoplasia in situ NG Embryonal carcinoma Endodermal sinus tumor Gonadoblastoma Teratoma Choriocarcinoma Embryoma Prostate Adenocarcinoma High-grade prostatic intraepithelial neoplasia HGPIN Small-cell carcinoma Transitional cell carcinoma Penis Carcinoma Extramammary Paget's disease Bowen's disease Bowenoid papulosis Erythroplasia of Queyrat Hirsuties coronae glandisH3P13, POU5F1P3, CDKN2A, F9, POU5F1, IL23A, REG1A, TP53, POU5F1P4, CDKN2D, SOX2, TNFRSF8, NANOG, DNMT3B, SLC22A3, AFP, EGFR, PODXL, DNMT3L, TDGF1, MDM2, SOX17, TDGF1P3, NM, PLSCR4, CCND2, CDKN1B, TRRAP, NOTCH1, KIT, FGF4, HSP90B1, PRAME, MIB1, BMP2, TH, BOC, LIF, NRIP1, TP63, DDX3Y, UTF1, FZD7, MIR371A, DLK1, UBE3B, ZNF202, HMGA2, GHS, TNFRSF10A, XIST, VIM, VCP, JPX, UVRAG, TPD52, SPANXA2, ESRG, TGFBR2, LEFTY2, TGFB2, TNFRSF10B, STK17A, MIR302B, NOLC1, CGB5, PRDM14, TSKS, SINHCAF, CGB8, SLAMF7, ZFP42, EMB, KDM3A, MEG3, DDX4, FXYD5, MYOZ2, CKS1BP7, SPANXA1, CD274, IGHV1-12, MAPK15, CBX7, RAB3GAP1, CLSTN1, CBX3, CHEK2, RASSF1, CKAP4, CIB1, GDF3, PHGDH, ABL1, ZNF354A, FGF9, DES, DNMT1, DRD2, ERF, ETV6, FGF2, FOXO1, CSH2, FN1, NR5A1, FUT4, GAP43, GSTP1, GTF2A1, DAXX, CSH1, HDAC1, CDH1, ALPL, FAS, ATRX, BRAF, CASP8, TNFSF8, CDK4, KLF6, CENPA, CGB3, RCC1, CHGB, CISH, CKS1B, GTF2A2, HLA-A, TCF3, RBL2, PSMD10, PTCH1, PTEN, MOK, RARB, RARG, ACTB, NODAL, CXCL12, SKP2, SLC5A5, SPAG1, ITPRID2, TBP, PCNA, NME2, HMGA1, KRT7, HPX, HTC2, IFNB1, IGF2, JAG2, KRAS, KRT18, NCL, LCN2, MCL1, MKI67, MOS, MTTP, MYD88, RPE65

-
Y Chromosome Microdeletion
Wikipedia
Y chromosome microdeletion (YCM) is a family of genetic disorders caused by missing gene(s) in the Y chromosome . Many men with YCM exhibit no symptoms and lead normal lives. ... Diagnosis [ edit ] Y chromosome microdeletion is currently diagnosed by extracting DNA from leukocytes in a man's blood sample, mixing it with some of the about 300 known genetic markers for sequence-tagged sites (STS) on the Y chromosome, and then using polymerase chain reaction amplification and gel electrophoresis in order to test whether the DNA sequence corresponding to the selected markers is present in the DNA. ... PMID 16157049 . ^ Poongothai J, Gopenath TS, Manonayaki S (April 2009). "Genetics of human male infertility" (PDF) .
-
Lymphomatoid Papulosis
Wikipedia
Archived from the original on 2011-05-24. ^ Neal S. Young; Stanton L. Gerson; Katherine A. ... Pathol . 125 (4): 490–501. doi : 10.1309/NNV4-L5G5-A0KF-1T06 . PMID 16627259 . ^ Dalle S, Balme B, Thomas L (2006). "Lymphomatoid papulosis localized to the face" . ... External links [ edit ] Classification D ICD - 10 : L41.2 ICD-O : 9718/1 MeSH : D017731 DiseasesDB : 33778 SNOMED CT : 31047003 External resources eMedicine : derm/254 Orphanet : 98842 v t e Leukaemias , lymphomas and related disease B cell ( lymphoma , leukemia ) (most CD19 CD20 ) By development/ marker TdT+ ALL ( Precursor B acute lymphoblastic leukemia/lymphoma ) CD5 + naive B cell ( CLL/SLL ) mantle zone ( Mantle cell ) CD22 + Prolymphocytic CD11c+ ( Hairy cell leukemia ) CD79a + germinal center / follicular B cell ( Follicular Burkitt's GCB DLBCL Primary cutaneous follicle center lymphoma ) marginal zone / marginal zone B-cell ( Splenic marginal zone MALT Nodal marginal zone Primary cutaneous marginal zone lymphoma ) RS ( CD15 +, CD30 +) Classic Hodgkin lymphoma ( Nodular sclerosis ) CD20+ ( Nodular lymphocyte predominant Hodgkin lymphoma ) PCDs / PP ( CD38 +/ CD138 +) see immunoproliferative immunoglobulin disorders By infection KSHV ( Primary effusion ) EBV Lymphomatoid granulomatosis Post-transplant lymphoproliferative disorder Classic Hodgkin lymphoma Burkitt's lymphoma HCV Splenic marginal zone lymphoma HIV ( AIDS-related lymphoma ) Helicobacter pylori ( MALT lymphoma ) Cutaneous Diffuse large B-cell lymphoma Intravascular large B-cell lymphoma Primary cutaneous marginal zone lymphoma Primary cutaneous immunocytoma Plasmacytoma Plasmacytosis Primary cutaneous follicle center lymphoma T/NK T cell ( lymphoma , leukemia ) (most CD3 CD4 CD8 ) By development/ marker TdT+ : ALL ( Precursor T acute lymphoblastic leukemia/lymphoma ) prolymphocyte ( Prolymphocytic ) CD30+ ( Anaplastic large-cell lymphoma Lymphomatoid papulosis type A ) Cutaneous MF+variants indolent: Mycosis fungoides Pagetoid reticulosis Granulomatous slack skin aggressive: Sézary disease Adult T-cell leukemia/lymphoma Non-MF CD30 -: Non-mycosis fungoides CD30− cutaneous large T-cell lymphoma Pleomorphic T-cell lymphoma Lymphomatoid papulosis type B CD30 +: CD30+ cutaneous T-cell lymphoma Secondary cutaneous CD30+ large-cell lymphoma Lymphomatoid papulosis type A Other peripheral Hepatosplenic Angioimmunoblastic Enteropathy-associated T-cell lymphoma Peripheral T-cell lymphoma not otherwise specified ( Lennert lymphoma ) Subcutaneous T-cell lymphoma By infection HTLV-1 ( Adult T-cell leukemia/lymphoma ) NK cell / (most CD56 ) Aggressive NK-cell leukemia Blastic NK cell lymphoma T or NK EBV ( Extranodal NK-T-cell lymphoma / Angiocentric lymphoma ) Large granular lymphocytic leukemia Lymphoid+ myeloid Acute biphenotypic leukaemia Lymphocytosis Lymphoproliferative disorders ( X-linked lymphoproliferative disease Autoimmune lymphoproliferative syndrome ) Leukemoid reaction Diffuse infiltrative lymphocytosis syndrome Cutaneous lymphoid hyperplasia Cutaneous lymphoid hyperplasia with bandlike and perivascular patterns with nodular pattern Jessner lymphocytic infiltrate of the skin General Hematological malignancy leukemia Lymphoproliferative disorders Lymphoid leukemias v t e Papulosquamous disorders Psoriasis Pustular Generalized pustular psoriasis ( Impetigo herpetiformis ) Acropustulosis / Pustulosis palmaris et plantaris ( Pustular bacterid ) Annular pustular psoriasis Localized pustular psoriasis Other Guttate psoriasis Psoriatic arthritis Psoriatic erythroderma Drug-induced psoriasis Inverse psoriasis Napkin psoriasis Seborrheic-like psoriasis Parapsoriasis Pityriasis lichenoides ( Pityriasis lichenoides et varioliformis acuta , Pityriasis lichenoides chronica ) Lymphomatoid papulosis Small plaque parapsoriasis ( Digitate dermatosis , Xanthoerythrodermia perstans ) Large plaque parapsoriasis ( Retiform parapsoriasis ) Other pityriasis Pityriasis rosea Pityriasis rubra pilaris Pityriasis rotunda Pityriasis amiantacea Other lichenoid Lichen planus configuration Annular Linear morphology Hypertrophic Atrophic Bullous Ulcerative Actinic Pigmented site Mucosal Nails Peno-ginival Vulvovaginal overlap synromes with lichen sclerosus with lupus erythematosis other: Hepatitis-associated lichen planus Lichen planus pemphigoides Other Lichen nitidus Lichen striatus Lichen ruber moniliformis Gianotti–Crosti syndrome Erythema dyschromicum perstans Idiopathic eruptive macular pigmentation Keratosis lichenoides chronica Kraurosis vulvae Lichen sclerosus Lichenoid dermatitis Lichenoid reaction of graft-versus-host disease
-
Amalgam Tattoo
Wikipedia
Low chronic inflammatory changes in the form of a lymphocytic aggregate (bottom right) Silver sulfide deposits are found in proximity to small vessels in the oral mucosa Silver sulfide deposits in the surrounding area of skeletal muscle fibers of the oral mucosa Amalgam tattoo usually occurs on the mandibular gingiva, often in an area in which an apicoectomy ("root-end filling") with amalgam was carried out. [3] : 138 After the gingiva, the alveolar mucosa and the buccal mucosa are the next most common sites, although any mucosal site in the mouth is possible. [1] It is painless, and appears as a blue-black or grey discolored macule on the surface of the mucosa. [3] : 138 [4] : 330 [5] : 183 The borders of the tattoo are variable, and may be well defined, irregular or diffuse. [1] Causes [ edit ] Amalgam tattoo is caused by implantation of amalgam into the tissues. [5] : 183 It may occur in several ways: During placement of an amalgam filling, [5] : 183 e.g. if abrasions on the mucosa are present which allow entry of amalgam dust [1] Shortly after placement of an amalgam filling, e.g. amalgam particles can contaminate dental floss and lead to linear amalgam tattoos in between the teeth, especially if flossing is carried out immediately after placement of an amalgam filling with a mesial or distal aspect [1] Polishing of an amalgam filling The pressure from high speed turbine dental drills can be enough to force amalgam particles into soft tissue, [1] as may occur when an old amalgam filling is being removed When a tooth with an amalgam filling is extracted, [5] : 183 e.g. broken bits of amalgam filling falling into an extraction socket unnoticed [1] When an amalgam filling is placed in the same appointment as a tooth extracted, as may occur in " quadrant dentistry " Apicectomies are common causes of amalgam tattoo, since the amalgam is being placed inside the alveolus and the soft tissues are replaced on top [1] Over time, the amalgam particles embedded in the soft tissues corrode. [5] : 183 Macrophages take up the exogenous particles, and the silver in amalgam leads to staining of collagen fibers . [5] : 183 A similar appearance can be caused by implantation of graphite (e.g. from pencil leads), and is sometimes termed a graphite tattoo , although this is less common than tattooing with amalgam. [3] : 138 Diagnosis [ edit ] The diagnosis is clinical. [3] : 138 Amalgam tattoo can be distinguished from other causes of localized oral pigmentation because it does not change significantly in size or color, [3] : 138 although it may appear to slowly enlarge for several months after the initial implantation of the metal particles. [1] [5] : 183 Some amalgam tattoos appear radio-opaque on radiographs (i.e. they show up on x-rays), [3] : 138 although in many cases amalgam tattoos have no radiographic features since the responsible particle(s) of amalgam are very small even though clinically the area of discolored mucosa is much larger. [1] If necessary, the diagnosis can be confirmed histologically by excisional biopsy , which excludes nevi and melanomas . [3] : 138 If a biopsy is taken, the histopathologic appearance is: [1] Pigmented fragments of metal within connective tissue Staining of reticulin fibers with silver salts A scattered arrangement of large, dark, solid fragments or a fine, black or dark brown granules Large particles may be surrounded by chronically inflamed fibrous tissue Smaller particles surrounded by more significant inflammation, which may be granulomatous or a mixture of lymphocytes and plasma cells Prevention [ edit ] Theoretically, routine use of a dental dam during dental procedures which involve amalgam should reduce the risk of amalgam tattoo. [1] Treatment [ edit ] No treatment is required since the lesion is entirely benign. ... Edinburgh: Churchill Livingstone/Elsevier. ISBN 9780443068966 . ^ a b Martin S. Greenberg; Michael Glick; Jonathan A.

-
Traumatic Aortic Rupture
Wikipedia
There can be bruising of the anterior chest wall, and a systolic murmur can be heard on the bottom of the heart. [5] Causes [ edit ] The injury is usually caused by high speed impacts such as those that occur in vehicle collisions and serious falls. [1] It may be due to different rates of deceleration of the heart and the aorta, which is in a fixed position. [6] Location of rupture [ edit ] By far the most common site for tearing in traumatic aortic rupture is the proximal descending aorta , near where the left subclavian artery branches off from the aorta. [7] The tethering of the aorta by the ligamentum arteriosum makes the site prone to shearing forces during sudden deceleration. [8] A study of people who died after traumatic aortic rupture found that in 55–65% of cases the damage was at the aortic isthmus and in 10–14% it was in the ascending aorta or aortic arch . [4] An angiogram will often show an irregular outpouching beyond the takeoff of the left subclavian artery at the aortic isthmus, representing an aortic pseudoaneurysm caused by the trauma. ... PMID 9927395 . ^ a b Plummer D, Petro K, Akbari C, O'Donnell S (2006). "Endovascular repair of traumatic thoracic aortic disruption". ... Belg . 88 (1): 33–38. PMID 3376665 . ^ Attar S, Cardarelli MG, Downing SW, et al. (1999).

-
Ulnar Neuropathy
Wikipedia
Ulnar neuropathy may be caused by entrapment of the ulnar nerve with resultant numbness and tingling . [3] Motor function can be assessed by testing for a positive Froment's sign , or making an OK sign (which the individual will be unable to do), little finger abduction can be tested as well. [ medical citation needed ] Contents 1 Signs and symptoms 2 Causes 3 Pathophysiology 4 Diagnosis 5 Treatment 6 Prognosis 7 References 8 Further reading 9 External links Signs and symptoms [ edit ] In terms of the signs/symptoms of ulnar neuropathy trauma and pressure to the arm and wrist, especially the elbow, the medial side of the wrist, and other sites close to the course of the ulnar nerve are of interest in this condition. ... Complaints of pain tend to be more common in the arm, up to and including the elbow area, which is probably the most common site of pain in an ulnar neuropathy. [1] [2] Causes [ edit ] Among the causes of ulnar neuropathy are the following- Olecranon Olecranon fractures [4] Distal humerus fractures [4] Medial epicondylar fractures [4] Valgus stress [4] Childhood supracondylar fracture [4] Transient occlusion brachial artery (surgery) [2] Subdermal contraceptive (implant) [2] Hemophilia [2] Tumor [2] Blunt injuries [2] Much more commonly, ulnar neuropathy is caused by overuse of the triceps muscle and repetitive stress combined with poor ergonomics. ... PMID 11883427 . ^ Apprill, P; Schmitz, JM; Campbell, WB; Tilton, G; Ashton, J; Raheja, S; Buja, LM; Willerson, JT (August 1985). ... Yoon, Joon Shik; Walker, Francis O.; Cartwright, Michael S. (1 February 2010). "Ulnar Neuropathy With Normal Electrodiagnosis and Abnormal Nerve Ultrasound" .

-
Paratuberculosis
Wikipedia
Intestinal disease has also been reported in rabbits and nonhuman primates. [ citation needed ] Unlike cattle and sheep, infections in deer often present with clinical illness in animals under one year of age. [ citation needed ] Pathophysiology [ edit ] The primary site targeted by Johne's disease is the lower part of the intestine known as the ileum . ... How M. paratuberculosis neutralizes or evades the normally efficient bacterial killing mechanisms of the macrophages is unknown, although the unusually resistant cell wall of mycobacteria likely plays an important role. [ citation needed ] The animal's immune system reacts to the M. paratuberculosis invasion by recruiting more macrophages and lymphocytes to the site of the infection. The lymphocytes release a variety of chemicals signals, called cytokines , in an attempt to increase the bacterial killing power of the macrophages. ... In the Merck Veterinary Manual, 8th ed. Edited by S. E. Aiello. Whitehouse Station, NJ: Merck and Co. 1998. ^ Richter, E., Wessling, J., Lügering, N., Domschke, W., & Rüsch-Gerdes, S. (2002).AOC3, C1R, C3, F2, TF, GSN, SLC11A1, SGSM3, NOD2, FN1, TLR4, NT5C3A, ANXA2, MNAT1, IL10, IFNG, SLC30A10, H3C9P, SLC30A8, IBD5, ST18, TLR2, MIR27A, IRGM, CCN6, CDK5R1, PHGDH, ATG16L1, LAMP3, AGO2, CDCA5, CD274, VSX1, NTM, ANXA1, RNR1, SLC22A4, CXCL8, ARSA, BGLAP, CAMP, CAT, DAG1, ENPEP, FCN2, GCHFR, HPD, HSPD1, IL10RA, RELA, IL12A, IL12B, IDO1, INS, IRF5, LSAMP, LYZ, MBP, MYD88, PTGS2, UPK3B
-
Hemolytic Poikilocytic Anemia Due To Reduced Ankyrin Binding Sites
Omim
Agre et al. (1981) presented evidence for reduction in the number of high affinity ankyrin binding sites. The findings were consistent with an abnormal organization of band 3 (109270) in the membrane. ... Spectrin binding was normal and patients' ankyrin and spectrin (both radioiodinated) competed normally for the binding sites on normal red cell membranes. None of the individual components appeared to have abnormal thermal sensitivity. ... Inheritance - Autosomal dominant Misc - Improved by splenectomy Lab - Reduced ankyrin binding sites Heme - Hemolytic anemia - Poikilocytosis - Elliptocytosis ▲ Close
-
Insulin Receptor Substrate 1
Omim
Peptide inhibition experiments using phosphoserine-containing peptides of IRS1 revealed that IRS1 contains 3 putative binding sites for 14-3-3 protein. Among these 3, the motif around serine-270 is located in the phosphotyrosine-binding (PTB) domain of IRS1, which is responsible for the interaction with the insulin receptor (INSR; 147670). ... Overexpression of MIR126 inhibited cell growth in HEK293 and breast cancer cells by suppressing cycle cycle progression from G0/G1 to S phase. Zhang et al. (2008) identified a complementary site for MIR126 in the 3-prime UTR of IRS1, and in vitro luciferase assays confirmed that MIR126 targeted IRS1. ... Because of its central role in the signal transduction pathway, IRS1 is a candidate for the site of the defect in insulin action seen in patients with noninsulin-dependent diabetes mellitus (NIDDM; 125853). ... Of the 3 amino acid substitutions observed by Laakso et al. (1994), they found ser892 to gly the most 'interesting' since it abolishes one of the potential serine phosphorylation sites which is located immediately N-terminal to the only SH2-binding site of growth factor receptor-bound protein (GRB2; 108355) and thus could potentially influence some aspects of signal transduction and metabolic response to insulin.
-
Health Effects Of Coal Ash
Wikipedia
Exposure to coal ash and to the toxic substances it contains may pose a health risk to workers in coal-fired power plants and residents living near coal ash disposal sites. Contents 1 Background 2 Occupational health concerns 3 Health effects of toxic constituents found in coal ash 4 Coal ash reuse 5 Coal ash waste regulations 6 References Background [ edit ] Coal ash is produced at coal-fired power plants . [1] Coal is pulverized and then burned to generate electricity. [2] The particles that remain after burning coal are called coal ash, principally consisting of fly ash and bottom ash . Other coal combustion by-products are boiler slag, flue gas desulfurization gypsum, and other kinds of flue gas desulfurization residues. [1] Depending on the type of coal that was burned, the chemical composition found in coal ash can vary. [3] Coal ash obtained from the combustion of bituminous coal is constituted principally of aluminum oxide (Al 2 O 3 ), calcium oxide (CaO) and silicon dioxide (SiO 2 ). [3] In the composition of coal, there are many potentially hazardous substances that, if found at elevated concentration in inhaled particles, can cause major health problems in humans. [4] [5] Such constituents that are found at various concentrations in coal ash are arsenic , cadmium , chromium , cobalt , copper , lead , lithium , mercury , molybdenum , selenium , thallium and uranium . [4] [5] Coal ash in India has been stored in ash ponds and has contaminated surrounding land and water bodies. [6] In the United States approximately 110 million tons of coal ash were generated in 2012. [1] More than half of the coal ash produced in the US was dumped into ash ponds (surface impoundments; wet disposal) or landfills (dry disposal). [5] As of 2020 there are 310 active on-site landfills and 735 active on-site surface impoundments in the US. [7] Occupational health concerns [ edit ] Coal ash contains many toxic substances that may affect human health, if people are exposed to them above a certain concentration in the form of particulate matter. ... Arsenic : When high amounts of arsenic is inhaled or ingested through coal ash waste, diseases such as bladder cancer, skin cancer, kidney cancer and lung cancer can develop. [5] [11] Ultimately, exposure of arsenic over a long period of time can cause mortality. [5] Furthermore, low levels of arsenic exposure can cause irregular heartbeats, nausea, diarrhea, vomiting, peripheral neuropathy and vision impairment. [9] [5] Mercury : Chronic exposure of mercury from coal ash can cause harm to the nervous system. [5] When mercury is inhaled or ingested various health effects can occur such as vision impairment, seizures, numbness, memory loss and sleeplessness. [12] [13] Boron : When coal ash dust is inhaled, the exposure of boron can cause discomfort in the throat, nose and eye. [5] Moreover, when coal ash waste is ingested, boron exposure can be associated with kidney, liver, brain, and intestine impairment. [5] Molybdenum : When molybdenum is inhaled from coal ash dust, discomfort of the nose, throat, skin and eye can occur. [14] As a result, short-term molybdenum exposure can cause an increase of wheezing and coughing. [14] Furthermore, chronic exposure of molybdenum can cause loss of appetite, tiredness, headaches and muscle soreness. [5] [14] Thallium : The exposure of thallium in coal ash dust can cause peripheral neuropathy when inhaled. [5] Furthermore, when coal ash is ingested, thallium exposure can cause diarrhea and vomiting. [5] In addition, thallium exposure is also associated with heart, liver, lung and kidney complications. [5] Silica : When silica is inhaled from coal ash dust, fetal lung disease or silicosis can develop. [4] Furthermore, chronic exposure of silica can cause lung cancer. [4] In addition, exposure to silica over a period of time can cause loss of appetite, poor oxygen circulation, breathing complications and fever. [4] Coal ash reuse [ edit ] Reuse of coal ash benefits the environment by reducing the production of greenhouse gas and reducing the need to use virgin materials. [15] In addition, when coal ash is recycled, costs related to coal ash disposal sites are avoided. [5] [15] There are two forms of coal ash recycling: “encapsulated” and “unencapsulated." [5] [15] When coal ash is bound to other materials it is encapsulated. [5] For example, coal ash can be reused in making concrete, bricks and wallboards. [15] On the other hand, unencapsulated use of coal ash is when the ash is not bound to other materials (loose particulate or sludge form). [5] [15] An example of unencapsulated coal ash is distributing the ash on icy roads in the winter. [5] Even though reusing coal ash minimizes health effects in humans, health problems can still occur when coal ash is recycled. [5] Specifically, workers drilling or cutting encapsulated coal ash increase their risk of inhaling coal ash dust. [5] In addition, when unencapsulated coal ash is scattered on snowy streets in the winter, the loose ash can come in contact with ditches on the side of the road. [5] As a result, the toxins from coal ash can leach into surface water bodies as well as groundwater , which may be drinking water sources. [5] Therefore, both forms of recycled coal ash (encapsulated and unencapsulated) can cause serious health issues in humans. ... The court ruled that EPA failed to adequately address the problems with unlined ponds, many of which continue to leak into groundwater. [21] In 2019, the court agreed to a voluntary remand while allowing the 2020 compliance deadline for unlined ponds to stay in effect, pending further rulemaking. [22] EPA published a proposed rule on August 14, 2019 that would use location-based criteria, rather than a numerical threshold (i.e. impoundment or landfill size) that would require an operator to demonstrate minimal environmental impact so that a site could remain in operation. [23] In response to litigation on the 2015 regulation, EPA published a final RCRA regulation on August 28, 2020 requiring all unlined ash ponds to retrofit with liners or close by April 11, 2021. ... Retrieved 3 March 2016 . ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa Gottlieb, Barbara; Gilbert, Steven G.; Evans, Lisa Gollin.

-
Muscular Dystrophy, Becker Type
Omim
Mapping Kingston et al. (1983, 1984) found linkage of BMD with the cloned sequence L1.28 (designated DXS7 by the seventh Human Gene Mapping Workshop in Los Angeles; D = DNA, X = X chromosome, S = segment, 7 = sequence of delineation). ... Arikawa-Hirasawa et al. (1995) found an extremely short dystrophin resulting from a large deletion in a boy with severe muscular dystrophy. The entire actin-binding site at the N terminus was missing, although the protein was predicted to have a putative binding site for the dystrophin-associated glycoprotein and still could associate with the sarcolemmal membrane. ... Sequencing the regions flanking the insertion revealed a point mutation in intron 2 (300377.0083) that creates an AG dinucleotide consensus sequence for a splicing acceptor site, predicted to produce a novel exon structure that is then incorporated into dystrophin mRNA. Yagi et al. (2003) stated that the creation of a splice acceptor site by a single nucleotide change leading to an extra exon structure is a novel molecular mechanism in human disease. ... Tuffery-Giraud et al. (2005) reported 5 splice site mutations in the DMD gene in 5 patients with Becker muscular dystrophy.DMD, TGFB1, POSTN, CD4, CCL2, BEST1, CLCN1, DAG1, UTRN, SGCG, SGCA, CAPN3, TTN, FST, FKRP, DYSF, ACE, TNF, ELP1, CCL27, MGAM, HSPB3, RGN, TIMP2, LARGE1, VIPR1, ACTB, WNT16, LDB3, RSPO3, LINC01672, MIR31, MIR30C2, MIR30C1, ANO5, FAM168B, UHMK1, ASRGL1, TRIM32, CPED1, MMEL1, DANCR, NAT10, TPPP3, PDLIM3, ATRNL1, TIMP1, SHBG, TAZ, DECR1, HLA-DMB, GK, GH1, MSTN, GAA, FN1, DTNA, CTLA4, SLPI, CREB1, BMP6, ALDH7A1, ATHS, APRT, ALPP, ALOX15, HSPB1, HSPB2, LMNA, MB, SI, SHOX, ALOX12, SGCB, SELENOP, SALL1, PTH, PRL, PLXNB1, NOS1, MYF6, MSH2, MMP9, MLH1, MFAP1, H3P14
-
Pattern Hair Loss
Wikipedia
PMC 3026732 . PMID 21206086 . ^ a b c d Inui, S.; Itami, S. (2012). "Androgen actions on the human hair follicle: Perspectives". ... PMID 15901667 . ^ Ellis, J. A.; Panagiotopoulos, S.; Akdeniz, A.; Jerums, G.; Harrap, S. ... J.; Merrick, A. E.; Hamada, K.; Kato, S.; Jenner, T. J.; De Oliveira, I.; Messenger, A. ... PMID 19678603 . ^ Yoo, H. G.; Kim, J. S.; Lee, S. R.; Pyo, H. K.; Moon, H. I.; Lee, J. H.; Kwon, O. S.; Chung, J. H.; Kim, K. H.; Eun, H.SRD5A2, AR, ABCC2, SUPV3L1, VDR, ZFP36, MTHFR, TNFRSF10A, BRD4, ZDHHC13, HR, PRKAR1A, CRH, PARP1, RHOA, WNT10A, C1orf127, FAF1, MKLN1-AS, TBX15, HOXD-AS2, ARL17B, LINC01432, SSPN, SLC14A2, FAM53B, EMC2, HDAC9, EDAR, MAPT-AS1, DRAIC, DKK2, KLF15, MEMO1, RSPO2, KANSL1, MRPS22, LINC00670, LRMDA, OFCC1, DPY30, GORAB, SPPL2C, THADA, GORAB-AS1, EBF1, RUNX1, MAPT, MKLN1, EIF3E, OPHN1, IRF4, FGF5, AGA, EDA2R, KLK3, TGFB1, GGCT, CD200, DKK1, CTNNB1, IGF1, CD34, DPP4, CYP27B1, COX8A, CRP, COL17A1, CARD14, PRNP, NLRP3, FGF2, CDKN2A, MS4A1, CASP3, C4BPA, MIR223, MIR451A, MIR146B, BDNF, XIAP, AGXT, AGT, AKR1C4, IL1B, KRT20, VEGFA, PTPN1, SHBG, SRD5A1, PPARA, ABCB1, OTC, PRDX2, TGFB1I1, TLR4, TNF, TP53, WNT10B, GHR, NFE2L2, NCOA4, LEP, KRT5, ABCB6, DHRS9, IL17A, MMRN1, TBC1D9, PTGDS, HPGDS, TGFBR1













