London: British Medical Journal. ISBN 978-0-7279-0743-1 . ^ Haws, Rachel A; Yakoob, Mohammad; Soomro, Tanya; Menezes, Esme V; Darmstadt, Gary L; Bhutta, Zulfiqar A (1 January 2009).
Arlington, VA: American Psychiatric Publishing. 2013. p. 433. ISBN 978-0-89042-554-1 . ^ DSM-IV , American Psychiatric Association 1994, p. 502 ^ McCabe, Marita P. (29 May 2006).
Orthostatic hypotension is a drop in blood pressure that occurs when moving from a laying down (supine) position to a standing (upright) position. The word "orthostasis" means to stand up, so the condition is defined as low blood pressure (hypotension) that occurs upon standing. When standing up, gravity moves blood from the upper body to the lower limbs. As a result, there is a temporary reduction in the amount of blood in the upper body for the heart to pump (cardiac output), which decreases blood pressure. Normally, the body quickly counteracts the force of gravity and maintains stable blood pressure and blood flow.
International Journal of Hematology . 93 (2): 144–9. doi : 10.1007/s12185-011-0776-0 . PMC 3689295 . PMID 21279816 . ^ a b c d McCann KL, Baserga SJ (2013).
Tarsal tunnel syndrome is a nerve disorder that is characterized by pain in the ankle, foot, and toes. This condition is caused by compression of the posterior tibial nerve, which runs through a canal near the heel into the sole of the foot. When tissues around this nerve become inflamed, they can press on the nerve and cause the pain associated with tarsal tunnel syndrome.
Academic Press: 419–425. doi : 10.1016/b978-0-12-386454-3.00018-x . ISBN 9780123864550 . ^ a b Klarskov K, Gagnon H, Boudreault PL, Normandin C, Plancq B, Marsault E, et al.
Washington, DC: Environment Department of the World Bank. ISBN 978-0-8213-7237-1 . ^ Ngure, Francis M.; Reid, Brianna M.; Humphrey, Jean H.; Mbuya, Mduduzi N.; Pelto, Gretel; Stoltzfus, Rebecca J.
Journal of Neurology . 257 (4): 653–654. doi : 10.1007/s00415-009-5411-0 . ISSN 0340-5354 . PMID 19997925 . ^ a b c d e f Chomel, Bruno B.; Sun, Ben (January 26, 2011).
Philadelphia: Lippincott-Raven Publishers. pp. 233 . ISBN 978-0-397-55192-7 . This article contains text from the public domain document at http://www.ninds.nih.gov/health_and_medical/disorders/spasticity_doc.htm Douglas, Wallace M.; Bruce H Ross; Christine K.
Overview Impetigo (im-puh-TIE-go) is a common and highly contagious skin infection that mainly affects infants and young children. It usually appears as reddish sores on the face, especially around the nose and mouth and on the hands and feet. Over about a week, the sores burst and develop honey-colored crusts. Impetigo Impetigo starts as a reddish sore that ruptures, oozes for a few days and then forms a honey-colored crust. Sores mainly occur around the nose and mouth in infants and children. Treatment with antibiotics can limit the spread of impetigo to others.
Elsevier. pp. 443–201. doi : 10.1016/B978-008045382-8.00161-1 . ISBN 978-0-08-045382-8 . [ verification needed ] ^ "Reading: The Resistance Phenomenon in Microbes and Infectious Disease Vectors: Implications for Human Health and Strategies for Containment -- Workshop Summary - The National Academies Press" . nap.edu . [ verification needed ] ^ "Tolerance and Resistance to Drugs" .
A number sign (#) is used with this entry because of evidence that Leber congenital amaurosis-17 (LCA17) is caused by compound heterozygous mutation in the GDF6 gene (601147) on chromosome 8q22. For a general phenotypic description and a discussion of genetic heterogeneity of Leber congenital amaurosis (LCA), see LCA1 (204000). Clinical Features Asai-Coakwell et al. (2013) studied a female LCA patient with compound heterozygous mutations in the GDF6 gene who had vision limited to detection of hand motions, with an extinguished electroretinogram (ERG) typical of the LCA phenotype. She did not have other ocular or systemic phenotypes, but the authors noted that she had not undergone radiologic imaging to detect milder GDF6-induced skeletal disease. Evaluation of her clinically unaffected mother revealed a delayed rod b-wave implicit time on ERG; similarly, her apparently unaffected father showed reduced b-wave amplitude.
A number sign (#) is used with this entry because of evidence that Leber congenital amaurosis-12 (LCA12) is caused by homozygous mutation in the RD3 gene (180040) on chromosome 1q32. For a general phenotypic description and a discussion of genetic heterogeneity of LCA, see LCA1 (204000). Clinical Features Friedman et al. (2006) identified a sister and brother with Leber congenital amaurosis from a consanguineous Indian family. Both probands had had poor vision since birth. Nystagmus and atrophic lesions in the macular area with pigment migration were found on examination. Preising et al. (2012) reported a large consanguineous Kurdish family with LCA, in which 6 of 7 affected individuals were available for study.
A number sign (#) is used with this entry because of evidence that Leber congenital amaurosis-9 (LCA9) is caused by homozygous or compound heterozygous mutation in the NMNAT1 gene (608700) on chromosome 1p36. For a general discussion of the phenotypic and genetic heterogeneity in Leber congenital amaurosis, see LCA1 (204000). Description Early-onset neurodegeneration in the human retina can lead to Leber congenital amaurosis (LCA), the most severe human form of inherited photoreceptor-neuron degeneration resulting in congenital blindness, with an incidence of approximately 1 in 80,000 (summary by Koenekoop et al., 2012). NMNAT1 (608700) mutations consistently cause severe and rapidly progressive macular degeneration leading to severe central atrophy with an appearance of congenital macular coloboma in the neonatal period, as well as an unusual early-onset atrophy of the optic nerve (Perrault et al., 2012). Clinical Features Koenekoop et al. (2012) reexamined affected individuals from 8 families with Leber congenital amaurosis in whom they had identified mutations in the NMNAT1 gene (608700), which is ubiquitously expressed (see MOLECULAR GENETICS).
A number sign (#) is used with this entry because Leber congenital amaurosis-5 (LCA5) is caused by homozygous mutation in the gene encoding lebercilin (LCA5; 611408) on chromosome 6q14. For a general phenotypic description and a discussion of genetic heterogeneity of LCA, see LCA1 (204000). Clinical Features Dharmaraj et al. (2000) described a multigenerational kindred of Old Order River Brethren, a religious isolate descended from Swiss immigrants to America in the 1750s (Brechbill, 1972), segregating Leber congenital amaurosis. LCA in this kindred was not associated with multisystem abnormalities. Renal function remained normal. Neurologic and hepatic function were within normal limits.
A number sign (#) is used with this entry because of evidence that Leber congenital amaurosis-1 (LCA1) is caused by homozygous mutation in the gene encoding retinal guanylate cyclase (GUCY2D; 600179) on chromosome 17p13. Heterozygous mutation in the GUCY2D gene causes an allelic disorder, cone-rod dystrophy-6 (CORD6; 601777), and homozygous mutation in the same gene has also been found to cause autosomal recessive CORD (see 610777). Description Leber congenital amaurosis comprises a group of early-onset childhood retinal dystrophies characterized by vision loss, nystagmus, and severe retinal dysfunction. Patients usually present at birth with profound vision loss and pendular nystagmus. Electroretinogram (ERG) responses are usually nonrecordable. Other clinical findings may include high hypermetropia, photodysphoria, oculodigital sign, keratoconus, cataracts, and a variable appearance to the fundus (summary by Chung and Traboulsi, 2009).
Leber congenital amaurosis (LCA) is an eye disorder that primarily affects the retina . People with this condition typically have severe visual impairment beginning in infancy. Other features include photophobia , involuntary movements of the eyes (nystagmus), and extreme farsightedness. The pupils also do not react normally to light. Additionally, the cornea may be cone-shaped and abnormally thin ( keratoconus ). Franceschetti's oculo-digital sign is characteristic of Leber congenital amaurosis.
A number sign (#) is used with this entry because Leber congenital amaurosis-11 (LCA11) is caused by heterozygous mutation in the IMPDH1 gene (146690) on chromosome 7q32. Heterozygous mutation in the IMPDH1 gene can also cause retinitis pigmentosa-10 (RP10; 180105). Description Leber congenital amaurosis comprises a group of early-onset childhood retinal dystrophies characterized by vision loss, nystagmus, and severe retinal dysfunction. Patients usually present at birth with profound vision loss and pendular nystagmus. Electroretinogram (ERG) responses are usually nonrecordable. Other clinical findings may include high hypermetropia, photodysphoria, oculodigital sign, keratoconus, cataracts, and a variable appearance to the fundus (summary by Chung and Traboulsi, 2009).
A number sign (#) is used with this entry because of evidence that Leber congenital amaurosis-16 (LCA16) is caused by homozygous mutation in the KCNJ13 gene (603208) on chromosome 2q37. For a general phenotypic description and a discussion of genetic heterogeneity of Leber congenital amaurosis, see LCA1 (204000). Clinical Features Sergouniotis et al. (2011) studied a consanguineous Middle Eastern family in which 2 brothers had nystagmus at birth and were diagnosed with Leber congenital amaurosis shortly thereafter. Poor night vision and difficulty reading print from an early age was reported for both patients; gradual progression of visual problems affecting central and peripheral vision was also noted. Both patients had bilateral cataract surgery in their third decade. Funduscopy revealed significant pigment in the retinal pigment epithelium (RPE), in a configuration unlike that of typical retinitis pigmentosa (see 268000).
A number sign (#) is used with this entry because Leber congenital amaurosis-7 can be caused by heterozygous or homozygous mutation in the CRX gene (602225) on chromosome 19q13. Description Leber congenital amaurosis comprises a group of early-onset childhood retinal dystrophies characterized by vision loss, nystagmus, and severe retinal dysfunction. Patients usually present at birth with profound vision loss and pendular nystagmus. Electroretinogram (ERG) responses are usually nonrecordable. Other clinical findings may include high hypermetropia, photodysphoria, oculodigital sign, keratoconus, cataracts, and a variable appearance to the fundus (summary by Chung and Traboulsi, 2009). For a general description and a discussion of genetic heterogeneity of LCA, see 204000.
A number sign (#) is used with this entry because Leber congenital amaurosis-15 and juvenile retinitis pigmentosa are caused by homozygous or compound heterozygous mutation in the TULP1 gene (602280) on chromosome 6p21.3. Description Autosomal recessive childhood-onset severe retinal dystrophy is a heterogeneous group of disorders affecting rod and cone photoreceptors simultaneously. The most severe cases are termed Leber congenital amaurosis, whereas the less aggressive forms are usually considered juvenile retinitis pigmentosa (summary by Gu et al., 1997). Mutation in TULP1 can also cause a form of autosomal recessive retinitis pigmentosa (RP14; 600132). For a general phenotypic description and a discussion of the genetic heterogeneity of Leber congenital amaurosis, see LCA1 (204000); for retinitis pigmentosa, see 268000.
A number sign (#) is used with this entry because Leber congenital amaurosis-8 (LCA8) is caused by homozygous or compound heterozygous mutation in the CRB1 gene (604210) on chromosome 1q31. Homozygous or compound heterozygous mutation in CRB1 can also cause retinitis pigmentosa-12 (RP12; 600105). Description Leber congenital amaurosis comprises a group of early-onset childhood retinal dystrophies characterized by vision loss, nystagmus, and severe retinal dysfunction. Patients usually present at birth with profound vision loss and pendular nystagmus. Electroretinogram (ERG) responses are usually nonrecordable. Other clinical findings may include high hypermetropia, photodysphoria, oculodigital sign, keratoconus, cataracts, and a variable appearance to the fundus (summary by Chung and Traboulsi, 2009).
A number sign (#) is used with this entry because of evidence that Leber congenital amaurosis-6 (LCA6) is caused by homozygous or compound heterozygous mutation in the RPGRIP1 gene (605446) on chromosome 14q11. Description Leber congenital amaurosis comprises a group of early-onset childhood retinal dystrophies characterized by vision loss, nystagmus, and severe retinal dysfunction. Patients usually present at birth with profound vision loss and pendular nystagmus. Electroretinogram (ERG) responses are usually nonrecordable. Other clinical findings may include high hypermetropia, photodysphoria, oculodigital sign, keratoconus, cataracts, and a variable appearance to the fundus (summary by Chung and Traboulsi, 2009). For a general description and a discussion of genetic heterogeneity of LCA, see 204000.
A number sign (#) is used with this entry because of evidence that Leber congenital amaurosis-2 (LCA2) is caused by homozygous or compound heterozygous mutation in the RPE65 gene (180069) on chromosome 1p31. Mutations in this gene also cause retinitis pigmentosa (RP20; 613794). Description Leber congenital amaurosis comprises a group of early-onset childhood retinal dystrophies characterized by vision loss, nystagmus, and severe retinal dysfunction. Patients usually present at birth with profound vision loss and pendular nystagmus. Electroretinogram (ERG) responses are usually nonrecordable. Other clinical findings may include high hypermetropia, photodysphoria, oculodigital sign, keratoconus, cataracts, and a variable appearance to the fundus (summary by Chung and Traboulsi, 2009).
Leber congenital amaurosis (LCA) is a retinal dystrophy defined by blindness and responses to electrophysiological stimulation (Ganzfeld electroretinogram (ERG)) below threshold, associated with severe visual impairment within the first year of life. Epidemiology The prevalence of LCA is 1/50,000 - 1/33,000 live births and accounts for 5% of all retinal dystrophies and 20% of blindness in school age children. Clinical description LCA is characterized by severely reduced visual acuity (less or equal 20/400) or blindness within in the first year of life. Sluggish pupillary responses, roving eye movement, photophobia, high hyperopia, nystagmus, convergent strabismus, or keratoconus may occur depending on the genetic cause. The Franceschetti's oculo-digital sign, comprising eye poking, pressing, and rubbing is pathognomonic.
A number sign (#) is used with this entry because of evidence that Leber congenital amaurosis-10 (LCA10) is caused by homozygous or compound heterozygous mutations in the CEP290 gene (610142) on chromosome 12q21. Description Leber congenital amaurosis is a severe retinal dystrophy, causing blindness or severe visual impairment at birth or during the first months of life (summary by den Hollander et al., 2006). For a general phenotypic description and a discussion of genetic heterogeneity of Leber congenital amaurosis, see LCA1 (204000). Clinical Features Den Hollander et al. (2006) reported a consanguineous French Canadian family in which 4 sibs had Leber congenital amaurosis. The sibs were blind or severely visually impaired at birth. Two of the 4 experienced seizures but had no other neurologic symptoms.
Sorsby and Williams (1960) observed a family with multiple cases of retinal aplasia in which inheritance was autosomal dominant. 'Retinal aplasia' is the British term for what is called 'congenital amaurosis' on the continent. Much genetic heterogeneity exists as evidenced by the demonstration of both autosomal dominant and autosomal recessive forms. This disorder, which might be called an autosomal dominant form of Leber amaurosis congenita, must be very rare. Heckenlively (1988) reported a 6-generation family with a severe progressive retinal degeneration beginning in infancy.
Born in Blood: The Lost Secrets of Freemasonry . ISBN 978-0-87131-602-8 . ^ Nick Leys, If you bought this, you've already had bad luck , review of Nathaniel Lachenmayer's Thirteen: The World's Most Popular Superstition , Weekend Australian, 8–9 January 2005 ^ 2013 number plates to be changed to avoid ‘unlucky 13’ , Irish Independent , 24 August 2012 ^ "2013 Number Plates To Be Changed To Avoid 'Unlucky 13 ' " .
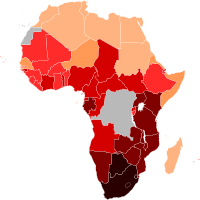
This program has resulted in greater access to treatment and a decrease in annual HIV- related deaths since the program's first implementation in 2006. [25] The largest source of international and domestic funds for HIV response comes from The Global Fund . [26] Impact on Vulnerable Populations [ edit ] Women and Children [ edit ] Estimated HIV prevalence among young adults (15-49) by country Women living with HIV/AIDS undergo a significant amount of obstacles due to socio-cultural constraints, and oftentimes gender norms prevent women from accessing healthcare services. [8] Additionally, infants are at risk of contracting the virus through mother-to-child transmission when HIV-positive mothers breastfeed without undergoing antiretroviral therapy. [27] A key study published in 2017 conducting HIV/AIDS research in Zimbabwe, Malawi , and Nigeria reports that "almost 80% of all infant infections [were] attributed to roughly 20% HIV-positive pregnant and breastfeeding women not retained on antiretroviral therapy." [27] However, progress has been made in recent years, as in 2015 the World Health Organization found that 93% of pregnant women had received antiretroviral treatment for the prevention of mother-to-child transmission, (also known as PMTCT ). [6] Furthermore, the number of children aged 0–14 living with the virus is estimated to be at 84,000 which is notably lower than men aged 15 and over living with HIV/AIDS (490,000) or women (730,000). [15] However, recent studies show that there are a variety of exceptions to these trends associated with socioeconomic status, as children in rural Zimbabwe that are "HIV-exposed and uninfected" have a 40% higher chance of death than other HIV-exposed children. [9] Sex Workers [ edit ] Sex workers in Zimbabwe face disproportionate levels of discrimination that impede their ability to access treatment options. [10] The majority of sex workers diagnosed with HIV/AIDS do not follow through with treatment options such as antiretroviral therapy upon diagnosis.