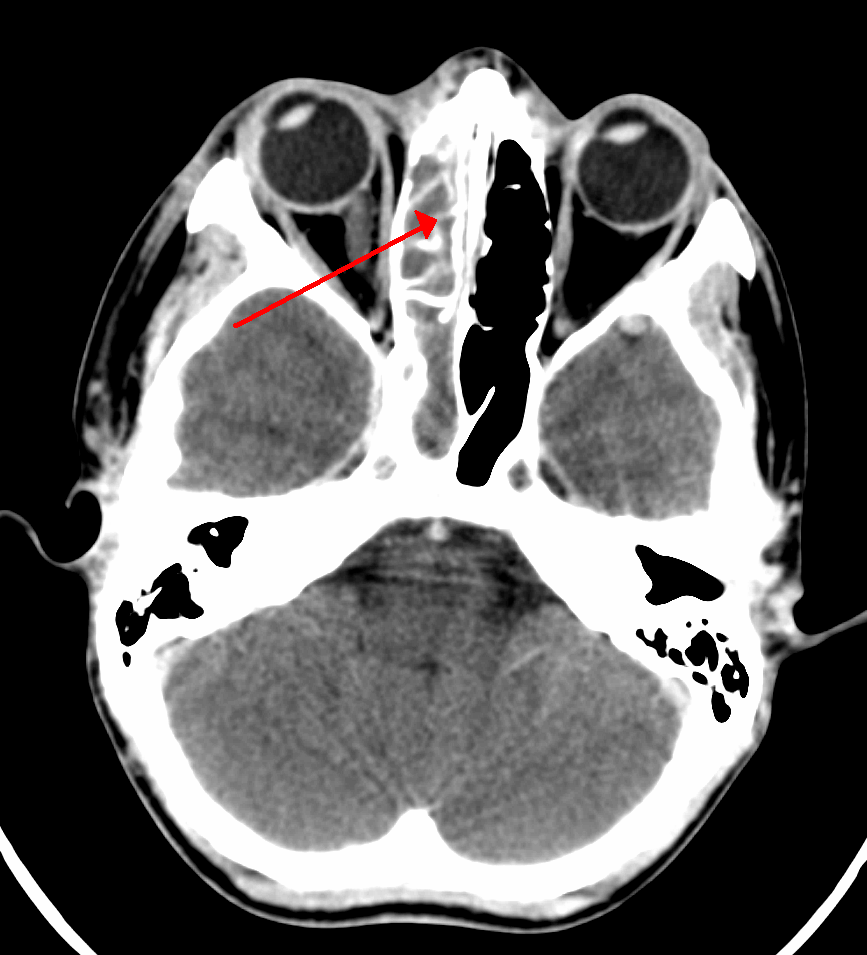
Carotid-cavernous fistula Other names CCF Oblique section through the cavernous sinus. Specialty Neurology , cardiology A carotid-cavernous fistula results from an abnormal communication between the arterial and venous systems within the cavernous sinus in the skull. ... As arterial blood under high pressure enters the cavernous sinus, the normal venous return to the cavernous sinus is impeded and this causes engorgement of the draining veins, manifesting most dramatically as a sudden engorgement and redness of the eye of the same side. ... Direct fistulas occur when the Internal Carotid artery (ICA) itself fistulizes into the Cavernous sinus whereas indirect is when a branch of the ICA or External Carotid artery (ECA) communicates with the cavernous sinus. ... Direct CCF may be treated by occlusion of the affected cavernous sinus (coils, balloon, liquid agents), or by reconstruction of the damaged internal carotid artery (stent, coils or liquid agents). ... PMID 22839357 . ^ Ong, CK; Wang, LL; Parkinson, RJ; Wenderoth, JD (2009). "Onyx embolisation of cavernous sinus dural arteriovenous fistula via direct percutaneous transorbital puncture".
Endodermal sinus tumor Other names Yolk sac tumor ( YST ) Micrograph showing the yolk sac component of a mixed germ cell tumour. ... In contrast to the pure form typical of infants, adult endodermal sinus tumors are often found in combination with other kinds of germ cell tumor, particularly teratoma and embryonal carcinoma . While pure teratoma is usually benign , endodermal sinus tumor is malignant . Contents 1 Cause 2 Diagnosis 2.1 Pathology 3 Treatment 4 See also 5 References 6 External links Cause [ edit ] Causes are poorly understood. ... Treatment with cisplatin , etoposide , and bleomycin has been described. [7] Before modern chemotherapy, this type of neoplasm was highly lethal, but the prognosis has significantly improved since then. [ citation needed ] When endodermal sinus tumors are treated promptly with surgery and chemotherapy, fatal outcomes are exceedingly rare. [8] See also [ edit ] Germ cell tumor Testicular cancer References [ edit ] ^ "Endodermal Sinus Tumor" . ... "Adjuvant chemotherapy in a pregnant woman with endodermal sinus tumor of the ovary". Obstetrics and Gynecology . 109 (2 Pt2): 537–40. doi : 10.1097/01.AOG.0000245450.62758.47 .
A rare germ cell tumor characterized by multiple patterns reflecting endodermal extraembryonal differentiation (secondary yolk sac and allantois) or endodermal somatic tissues (intestine, liver, and mesenchyme). The tumors most commonly occur in the second or third decade of life. They are typically located in the gonads, occasionally also in other regions. Patients present with a pelvic mass and/or abdominal pain (females) or an often painless, unilateral testicular mass (males). Elevated serum alpha fetoprotein is a common laboratory finding.
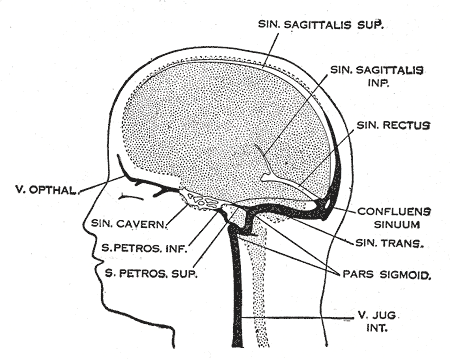
Anatomic types are the lateral type involving the jugular bulb, which presents with minimal symptoms, and the usually symptomatic midline type involving the confluens sinuum (torcular Herophili) and adjacent posterior sinuses. Complications include sinus thrombosis, venous infarction, and cerebral hemorrhage, as well as cardiac failure, macrocrania, and hydrocephalus.
Cerebral venous sinus thrombosis Other names Cerebral venous and sinus thrombosis, (superior) sagittal sinus thrombosis, dural sinus thrombosis, intracranial venous thrombosis, cerebral thrombophlebitis Dural veins Specialty Neurology Treatment Low molecular weight heparin [1] Cerebral venous sinus thrombosis ( CVST ) is the presence of a blood clot in the dural venous sinuses , which drain blood from the brain . ... D-dimer [ edit ] There is an association between the D-dimer blood test and cerebral venous sinus thrombosis. [7] This association however is not strong enough to rule out the diagnosis alone. [7] Further tests [ edit ] In most patients, the direct cause for the cerebral sinus thrombosis is not readily apparent. ... "Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT)" . ... PMID 20784169 . ^ Ray BS, Dunbar HS, Dotter CT (January 1951). "Dural sinus venography as an aid to diagnosis in intracranial disease". ... "Clinical guideline Cerebral Venous Sinus Thrombosis in Children" . Archived from the original on 2 February 2009 .
Most often this is due to ectopic beats occurring so frequently that there is one after each sinus beat , or normal heartbeat. The two beats are figuratively similar to two twins (hence bi- + gemini ). For example, in ventricular bigeminy, a sinus beat is shortly followed by a PVC, a pause, another normal beat, and then another PVC. [1] In atrial bigeminy, the other "twin" is a premature atrial contraction (PAC). ... Thus the atrium is not depolarized and the sinus node is not reset. Since the sinus p wave to PVC interval is less than the normal P-P interval, the interval between the PVC and the next p wave is prolonged to equal the normal time elapsed during two P-P intervals. ... This then allows for re-entrant circuits and sets up the ventricle for another PVC after the next sinus beat. [2] The constant interval between the sinus beat and PVC suggests a reentrant etiology rather than spontaneous automaticity of the ventricle. [3] Atrial premature complexes (APCs) do not have a compensatory pause since they reset the sinus node but atrial or supraventricular bigeminy can occur. If the APCs are very premature, the wavefront can encounter a refractory AV node and not be conducted. This can be mistaken for sinus bradycardia if the APC is buried in the T wave since the APC will reset the SA node and lead to a long P-P interval. [2] Diagnosis [ edit ] A rhythm strip demonstrating bigeminy simple ECG of a Supraventricular Bigeminy Rule of bigeminy [ edit ] When the atrial rhythm is irregular (as in atrial fibrillation or sinus arrythmia) the presence of bigeminy depends on the length of the P-P interval and happens more frequently with a longer interval.
Persistent left superior vena cava connecting to the left-sided atrium is a rare, congenital vascular malformation of the major vessels characterized by a persitent left superior vena cava which drains directly to the left atrium, without passing through the coronary sinus (that may be absent in some cases).
These phenotypes include bradycardia, sinus arrhythmia, delayed conduction/conduction block, idiopathic ventricular fibrillation, and catecholaminergic polymorphic ventricular tachycardia (Mohler et al., 2007). ... Since the initial description, Mohler et al. (2003) reported that 8 additional individuals had been born, of whom 4 carried the LQT4 haplotype. Sinus node abnormalities were diagnosed in utero in all affected members from generation 4. ... Mapping In a 65-member family in which the long QT syndrome was associated with more marked sinus bradycardia than usual, leading to sinus node dysfunction, Schott et al. (1995) excluded linkage to 3 previously mapped LQT loci on chromosomes 11 (LQT1; 192500), 7 (LQT2; 613688), and 3 (LQT3; 603830). ... Nomenclature Splawski (2004) suggested the designation 'sick sinus syndrome associated with bradycardia' for this disorder. ... INHERITANCE - Autosomal dominant CARDIOVASCULAR Heart - Prolong QT interval on EKG - Sinus bradycardia - Sinus nude dysfunction - Atrial fibrillation - Syncope - Sudden cardiac death MISCELLANEOUS - Genetic heterogeneity (see LQT1 192500 ) MOLECULAR BASIS - Caused by mutation in the ankyrin 2 gene (ANK2, 106410.0001 ) ▲ Close
Electrocardiogram intervals were similar in 6 of 21 +/+ and -/- mice; however, adult -/- mice manifested abrupt spontaneous episodes of sinus brachycardia. This phenomenon was never observed in +/+ mice. ... Lees-Miller et al. (2003) concluded that knockout of ERG1 B predisposes mice to episodic sinus brachycardia. In a porcine model of postmyocardial infarction ventricular tachycardia, Sasano et al. (2006) demonstrated that focal gene transfer of the dominant-negative mutant G628S (152427.0008) to the infarct scar border zone resulted in complete elimination of ventricular arrhythmia inducibility, showing that gene transfer can eliminate cardiac tachyarrhythmias in a clinically relevant disease model.
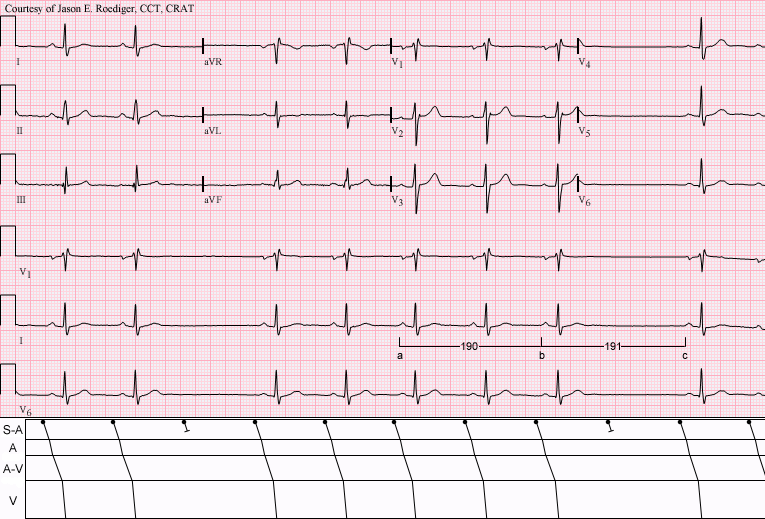
A number sign (#) is used with this entry because of evidence that long QT syndrome-10 (LQT10) and familial atrial fibrillation-17 (ATFB17) are caused by heterozygous mutation in the SCN4B gene (608256) on chromosome 11q23. For a discussion of genetic heterogeneity of long QT syndrome, see LQT1 (192500). For a discussion of genetic heterogeneity of familial atrial fibrillation, see ATFB1 (608583). Clinical Features Long QT Syndrome 10 Medeiros-Domingo et al. (2007) reported a 5-year-old Mexican mestizo girl who at 21 months of age was found to have asymptomatic bradycardia with rates less than 60 bpm. An ECG revealed profound QT prolongation with a QTc of 712 ms and intermittent 2:1 AV block; during 1:1 conduction, macroscopic T-wave alternans was observed.
Activity of 1795insD channels during SA node pacemaking was confirmed by action potential (AP) clamp experiments, and the previously characterized persistent inward current (I-pst) and negative shift were implemented into SA node (AP) models. The -10 mV shift decreased the sinus rate by decreasing the diastolic depolarization rate, whereas the I-pst decreased the sinus rate by AP prolongation, despite a concomitant increase in the diastolic depolarization rate. In combination, a moderate I-pst (1 to 2%) and the shift reduced the sinus rate by about 10%. Veldkamp et al. (2003) concluded that sodium channel mutations displaying an I-pst or a negative shift in inactivation may account for the bradycardia seen in LQT3 patients, whereas SA node pauses or arrest may result from failure of SA node cells to repolarize under conditions of extra net inward current. ... Makita et al. (2008) genotyped 66 members of 44 LQT3 families of multiple ethnicities and identified the E1784K mutation in the SCN5A gene (600163.0008) in 41 individuals from 15 (34%) of the kindreds; the diagnoses in these individuals included LQT3 syndrome, Brugada syndrome (601144), and/or sinus node dysfunction (see 608567). In vitro functional characterization of E1784K compared to properties reported for other LQT3 variants suggested that a negative shift of steady-state Na channel inactivation and enhanced tonic block in response to Na channel blockers represent common biophysical mechanisms underlying the phenotypic overlap of LQT3 and Brugada syndromes, and further indicated that class IC drugs should be avoided in patients with Na channels displaying these behaviors.
Marsman et al. (2014) studied a Moroccan family with 5 sibs in which the proband experienced cardiac arrest at age 16 years while romping with a classmate at school; an initial recorded rhythm of VF was converted to a sinus rhythm after 2 defibrillatory shocks.
A number sign (#) is used with this entry because of evidence that long QT syndrome-12 (LQT12) is caused by heterozygous mutation in the alpha-1 syntrophin gene (SNTA1; 601017) on chromosome 20q11. Description Congenital long QT syndrome (LQTS) is electrocardiographically characterized by a prolonged QT interval and polymorphic ventricular arrhythmias (torsade de pointes). These cardiac arrhythmias may result in recurrent syncope, seizure, or sudden death (Jongbloed et al., 1999). For a discussion of genetic heterogeneity of long QT syndrome, see LQT1 (192500). Molecular Genetics Ueda et al. (2008) analyzed the SNTA1 gene in 50 unrelated patients with long QT syndrome who were negative for mutations in the 11 known LQTS genes and identified a heterozygous missense mutation (A390V; 601017.0001) in 1 patient.
Digenic Inheritance Vatta et al. (2006) identified a long QT syndrome patient who had biallelic digenic mutations: a 14-year-old girl with nonexertional syncope and a 'seizure-like' presentation, who had U waves, sinus bradycardia, and a QTc of 405 ms on ECG, was found to carry a missense mutation in the LQT2-associated KCNH2 gene as well as a mutation in the CAV3 gene (see 601253.0018 and 152427.0024). INHERITANCE - Autosomal dominant CARDIOVASCULAR Heart - Prolongation of corrected QT interval - Nonexertional syncope (in some patients) - Sinus bradycardia (in some patients) - Cardiac arrest (in some patients) LABORATORY ABNORMALITIES - Marked increase in late sodium current on voltage-clamp studies MISCELLANEOUS - Sudden unexplained infant death (SIDS) reported in some patients MOLECULAR BASIS - Caused by mutation in the caveolin 3 gene (CAV3, 601253.0016 ) ▲ Close
A number sign (#) is used with this entry because long QT syndrome-1 (LQT1) is caused by heterozygous mutation in the KQT-like voltage-gated potassium channel-1 gene (KCNQ1; 607542) on chromosome 11p15. Digenic inheritance has also been reported; see MOLECULAR GENETICS. Description Congenital long QT syndrome is electrocardiographically characterized by a prolonged QT interval and polymorphic ventricular arrhythmias (torsade de pointes). These cardiac arrhythmias may result in recurrent syncope, seizure, or sudden death (Jongbloed et al., 1999). A form of torsade de pointes in which the first beat has a short coupling interval has been described (613600). Genetic Heterogeneity of Long QT Syndrome Other forms of LQT syndrome (LQTS) are LQT2 (613688), caused by mutation in the KCNH2 gene (152427); LQT3 (603830), caused by mutation in the SCN5A gene (600163); LQT4 (see 600919), caused by mutation in the ANK2 gene (106410); LQT5 (613695), caused by mutation in the KCNE1 gene (176261); LQT6 (613693), caused by mutation in the KCNE2 gene (603796); LQT7 (Andersen cardiodysrhythmic periodic paralysis, 170390), caused by mutation in the KCNJ2 gene (600681); LQT8 (618447), caused by mutation in the CACNA1C gene (114205); LQT9 (611818), caused by mutation in the CAV3 gene (601253); LQT10 (611819), caused by mutation in the SCN4B gene (608256); LQT11 (611820), caused by mutation in the AKAP9 gene (604001); LQT12 (612955), caused by mutation in the SNTA1 gene (601017); LQT13 (613485), caused by mutation in the KCNJ5 gene (600734); LQT14 (616247), caused by mutation in the CALM1 gene (114180), and LQT15 (616249), caused by mutation in the CALM2 gene (114182).
Congenital long QT syndrome (LQTS) is a hereditary cardiac disease characterized by a prolongation of the QT interval at basal ECG and by a high risk of life-threatening arrhythmias. Epidemiology Disease prevalence is estimated at close to 1 in 2,500 live births. Clinical description The two cardinal manifestations of LQTS are syncopal episodes, which may lead to cardiac arrest and sudden cardiac death, and electrocardiographic abnormalities, including prolongation of the QT interval and T wave abnormalities. Etiology The genetic basis of the disease was identified in the mid-nineties and all the LQTS genes identified so far encode cardiac ion channel subunits or proteins involved in modulating ionic currents. Mutations in these genes ( KCNQ1 , KCNH2 , KCNE1 , KCNE2 , CACNA1c , CAV3 , SCN5A , SCN4B ) cause the disease by prolonging the duration of the action potential.
A number sign (#) is used with this entry because of evidence that long QT syndrome-5 (LQT5) is caused by heterozygous mutation in the KCNE1 gene (176261) on chromosome 21q22. Digenic inheritance has also been reported; see MOLECULAR GENETICS. Description Congenital long QT syndrome is electrocardiographically characterized by a prolonged QT interval and polymorphic ventricular arrhythmias (torsade de pointes). These cardiac arrhythmias may result in recurrent syncope, seizure, or sudden death (Jongbloed et al., 1999). For a discussion of genetic heterogeneity of long QT syndrome, see LQT1 (192500). Molecular Genetics In affected members of 2 families with long QT syndrome, Splawski et al. (1997) identified heterozygosity for different missense mutations in the KCNE1 gene (176261.0003-176261.0004).
A number sign (#) is used with this entry because of evidence that long QT syndrome-6 (LQT6) is caused by heterozygous mutation in the KCNE2 gene (603796) on chromosome 21q22. Digenic inheritance has also been reported; see MOLECULAR GENETICS. Description Congenital long QT syndrome is electrocardiographically characterized by a prolonged QT interval and polymorphic ventricular arrhythmias (torsade de pointes). These cardiac arrhythmias may result in recurrent syncope, seizure, or sudden death (Jongbloed et al., 1999). For a discussion of genetic heterogeneity of long QT syndrome, see LQT1 (192500). Clinical Features Abbott et al. (1999) reported a healthy 38-year-old Caucasian female who had had ventricular fibrillation while jogging.
A number sign (#) is used with this entry because of evidence that long QT syndrome-11 (LQT11) is caused by heterozygous mutation in the gene encoding the A-kinase anchor protein-9 (AKAP9; 604001) on chromosome 7q21. One such family has been reported. For a discussion of genetic heterogeneity of long QT syndrome, see LQT1 (192500). Description Congenital long QT syndrome is electrocardiographically characterized by a prolonged QT interval and polymorphic ventricular arrhythmias (torsade de pointes). These cardiac arrhythmias may result in recurrent syncope, seizure, or sudden death (Jongbloed et al., 1999). Molecular Genetics In a 13-year-old Caucasian girl with long QT syndrome, who was negative for mutation in the known LQT genes, Chen et al. (2007) identified heterozygosity for a ser1570-to-leu (S1570L; 604001.0001) substitution in the AKAP9 gene.
Overview Sinus headaches are headaches that may feel like an infection in the sinuses (sinusitis). ... In fact, studies have shown that most people who see a health care provider for sinus headaches are found to have migraines instead. ... Sinus headaches are associated with pain and pressure in the face and sinuses and can cause nasal symptoms. Most of these headaches are not caused by sinus infections and generally should not be treated with antibiotics. ... Treatment Most people who assume they have sinus headaches actually have migraines or tension-type headaches.
Find sources: "Sinoatrial block" – news · newspapers · books · scholar · JSTOR ( January 2016 ) ( Learn how and when to remove this template message ) Sinoatrial block Sinus rhythm (rate = 65/min) with Type II S-A (exit) block; (see laddergram). ... The p-cells in the centre of the node produce the rhythm at a regular rate, but their conduction across the node to where it meets atrial tissue is where the slowing occurs. A second degree type II, or sinus exit block, is a regular rhythm that may be normal or slow. ... A third degree sinoatrial block looks very similar to a sinus arrest. However, a sinus arrest is caused by a failure to form impulses. ... The pause ends with a P wave, instead of a junctional escape beat the way a sinus arrest would. Treatment [ edit ] Emergency treatment consists of administration of atropine sulfate or transcutaneous pacing . ... External links [ edit ] Classification D ICD - 10 : I45.5 ICD - 9-CM : 426.6 MeSH : D012848 v t e Anatomy of the heart General Surface base apex sulci coronary interatrial anterior interventricular posterior interventricular borders right left Internal atria interatrial septum pectinate muscles terminal sulcus ventricles interventricular septum trabeculae carneae chordae tendineae papillary muscle valves cusps atrioventricular septum cardiac skeleton intervenous tubercle Chambers Right heart ( venae cavae , coronary sinus ) → right atrium ( atrial appendage , fossa ovalis , limbus of fossa ovalis , crista terminalis , valve of inferior vena cava , valve of coronary sinus ) → tricuspid valve → right ventricle ( infundibulum , moderator band/septomarginal trabecula , crista supraventricularis ), → pulmonary valve → ( pulmonary artery and pulmonary circulation ) Left heart ( pulmonary veins ) → left atrium ( atrial appendage ) → mitral valve → left ventricle → aortic valve ( aortic sinus ) → ( aorta and systemic circulation ) Layers Endocardium heart valves Myocardium Conduction system cardiac pacemaker SA node Bachmann's bundle AV node bundle of His bundle branches Purkinje fibers Pericardial cavity pericardial sinus Pericardium fibrous pericardium sternopericardial ligaments serous pericardium epicardium/visceral layer fold of left vena cava Blood supply Circulatory system Coronary circulation Coronary arteries
Sinus [ edit ] Atrial bradycardias are divided into three types. The first, respiratory sinus arrhythmia , is usually found in young and healthy adults. ... This is thought to be caused by changes in the vagal tone during respiration. [5] If the decrease during exhalation drops the heart rate below 60 BPM on each breath, this type of bradycardia is usually deemed benign and a sign of good autonomic tone . The second, sinus bradycardia , is a sinus rhythm of less than 60 BPM. ... Studies have found that 50–85% of conditioned athletes have benign sinus bradycardia, as compared to 23% of the general population studied. [6] The heart muscle of athletes has become conditioned to have a higher stroke volume , so requires fewer contractions to circulate the same volume of blood. [5] The third, sick sinus syndrome , covers conditions that include severe sinus bradycardia, sinoatrial block , sinus arrest , and bradycardia-tachycardia syndrome ( atrial fibrillation , atrial flutter , and paroxysmal supraventricular tachycardia ). [5] Atrioventricular junction [ edit ] An AV-junctional rhythm , or atrioventricular nodal bradycardia, is usually caused by the absence of the electrical impulse from the sinus node . ... An AV-junctional escape complex is a normal response that may result from excessive vagal tone on the SA node. Pathological causes include sinus bradycardia, sinus arrest, sinus exit block, or AV block. [5] Ventricular [ edit ] Idioventricular rhythm , also known as atrioventricular bradycardia or ventricular escape rhythm, is a heart rate of less than 50 BPM.
Within the upper right chamber of the heart (right atrium) is a group of cells called the sinus node. The sinus node is the heart's natural pacemaker. ... Bradycardia occurs when these signals slow down or are blocked. Sinus node problems Bradycardia often starts in the area of the heart called the sinus node. In some people, sinus node problems cause alternating slow and fast heart rates (bradycardia-tachycardia syndrome).
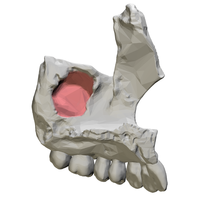
Symptoms [ edit ] · Same side nose blockage (unilateral nasal obstruction). [2] When an OAC or OAF is present, the passage to the maxillary sinus can results in infection and inflammation in the maxillary sinus. ... Pain can be referred to the upper teeth and be mistaken for toothache [3] · Fluid can flow from the mouth through the communication and into the maxillary sinus. The maxillary sinus is connected to the nose and therefore fluid can come out of the nostrils when drinking [2] · Change in sounds produced from the nose and the voice – specifically a whistling sound whilst speaking [2] · Taste can be affected [2] Signs [ edit ] · Visible hole between mouth and sinus · Fracture of the floor of the maxillary sinus creating a communication to the oral cavity (e.g. as seen following trauma). [2] · Air bubbles, blood or mucoid secretion around the orifice can be seen as air passes from the sinus into the oral cavity through the communication. ... Assess for the presence of visible an opening/hole between the oral cavity and the maxillary sinus. - Imaging can be useful. However, radiographs only show if there is a breach in the bony floor of the antrum. ... For example: Candidal infection [9] [10] Chronic maxillary sinus infection of bacterial origin [11] Osteomyelitis [12] Rhinosinusitis [13] Sinus pathology [9] Therefore, OAF should be dealt with first, before treating the complications. ... Antibiotics can help control or prevent any sinus infections. Preoperative nasal decongestants usage can reduce any existing sinus inflammation which will aid surgical manipulation of the mucosa over the bone. [18] Postoperative care [ edit ] Following all methods of OAC/OAF closure, the patients are instructed to avoid activities that could produce pressure changes between the nasal passages and oral cavity for at least 2 weeks due to risk of disruption to the healing process.
Fixed ventricular parasystole occurs when an ectopic pacemaker is protected by entrance block, and thus its activity is completely independent from the sinus pacemaker activity. Hence, the ectopic pacemaker is expected to fire at a fixed rate. Therefore, on ECG , the coupling intervals of the manifest ectopic beats will wander through the basic cycle of the sinus rhythm . Accordingly, the traditional electrocardiographic criteria used to recognize the fixed form of parasystole are: the presence of variable coupling intervals of the manifest ectopic beats; inter-ectopic intervals that are simple multiples of a common denominator; fusion beats . ... Therefore, appropriate diagnosis of modulated parasystole relies upon the construction of a “ phase response curve ” as theoretical evidence of modulation of the ectopic pacemaker cycle length by the electrotonic activity generated by the sinus discharges across the area of protection. ... In this case, the coupling intervals between the manifest ectopic and sinus discharges will be either fixed or variable, depending on the cycle length relations between the two pacemakers. See also [ edit ] Extrasystole References [ edit ] External links [ edit ] Classification D MeSH : D017574 ventricular parasystole atrial parasystole v t e Cardiovascular disease (heart) Ischaemic Coronary disease Coronary artery disease (CAD) Coronary artery aneurysm Spontaneous coronary artery dissection (SCAD) Coronary thrombosis Coronary vasospasm Myocardial bridge Active ischemia Angina pectoris Prinzmetal's angina Stable angina Acute coronary syndrome Myocardial infarction Unstable angina Sequelae hours Hibernating myocardium Myocardial stunning days Myocardial rupture weeks Aneurysm of heart / Ventricular aneurysm Dressler syndrome Layers Pericardium Pericarditis Acute Chronic / Constrictive Pericardial effusion Cardiac tamponade Hemopericardium Myocardium Myocarditis Chagas disease Cardiomyopathy Dilated Alcoholic Hypertrophic Tachycardia-induced Restrictive Loeffler endocarditis Cardiac amyloidosis Endocardial fibroelastosis Arrhythmogenic right ventricular dysplasia Endocardium / valves Endocarditis infective endocarditis Subacute bacterial endocarditis non-infective endocarditis Libman–Sacks endocarditis Nonbacterial thrombotic endocarditis Valves mitral regurgitation prolapse stenosis aortic stenosis insufficiency tricuspid stenosis insufficiency pulmonary stenosis insufficiency Conduction / arrhythmia Bradycardia Sinus bradycardia Sick sinus syndrome Heart block : Sinoatrial AV 1° 2° 3° Intraventricular Bundle branch block Right Left Left anterior fascicle Left posterior fascicle Bifascicular Trifascicular Adams–Stokes syndrome Tachycardia ( paroxysmal and sinus ) Supraventricular Atrial Multifocal Junctional AV nodal reentrant Junctional ectopic Ventricular Accelerated idioventricular rhythm Catecholaminergic polymorphic Torsades de pointes Premature contraction Atrial Junctional Ventricular Pre-excitation syndrome Lown–Ganong–Levine Wolff–Parkinson–White Flutter / fibrillation Atrial flutter Ventricular flutter Atrial fibrillation Familial Ventricular fibrillation Pacemaker Ectopic pacemaker / Ectopic beat Multifocal atrial tachycardia Pacemaker syndrome Parasystole Wandering atrial pacemaker Long QT syndrome Andersen–Tawil Jervell and Lange-Nielsen Romano–Ward Cardiac arrest Sudden cardiac death Asystole Pulseless electrical activity Sinoatrial arrest Other / ungrouped hexaxial reference system Right axis deviation Left axis deviation QT Short QT syndrome T T wave alternans ST Osborn wave ST elevation ST depression Strain pattern Cardiomegaly Ventricular hypertrophy Left Right / Cor pulmonale Atrial enlargement Left Right Athletic heart syndrome Other Cardiac fibrosis Heart failure Diastolic heart failure Cardiac asthma Rheumatic fever This article about a medical condition affecting the circulatory system is a stub .
Pneumosinus dilatans Lateral view paranasal sinus Pneumosinus dilatans is a condition consisting of abnormal expansion or dilatation of one or more paranasal sinuses . It most often affects the frontal sinus, and can cause damage to vision due to pressure on the nearby optic nerve . The preferred treatment is endoscopic surgery to deflate the sinus. Sources [ edit ] Hsu, Wen-Ming; et al. (2002).
The pattern of PFHB2, however, tends to develop along the lines of a sinus bradycardia with a left posterior hemiblock, presenting clinically as syncopal episodes, Stokes-Adams seizures, or sudden death when complete heart block supervenes (Brink and Torrington, 1977). ... Of 24 family members who underwent electrocardiography, 10 had conduction abnormalities, including 3 with sinus bradycardia, 3 with isolated left posterior hemiblock, 1 with atrial fibrillation and a slow ventricular response, and 2 with complete heart block (the latter 2 had pacemakers implanted). ... Ten families had pure AV block, 6 had members with AV block or sinus bradycardia, and 3 had pure sinus bradycardia. ... INHERITANCE - Autosomal dominant CARDIOVASCULAR Heart - Sinus bradycardia - Atrioventricular nodal disease - Atrioventricular block - Idionodal escape rhythm - Complete heart block with narrow QRS complexes MISCELLANEOUS - Syncope - Stokes-Adams attacks - Sudden death ▲ Close
A genetic cardiac rhythm disease that may progress to complete atrioventricular (AV) block. The disease is either asymptomatic or manifests as dyspnea, dizziness, syncope, abdominal pain, heart failure or sudden death. Epidemiology To date more than 50 Familial progressive cardiac conduction defect (PCCD) cases have been described in the literature. Clinical description The age of disease onset is variable. Familial PCCD is either asymptomatic or manifests as dyspnea, dizziness, syncopal episodes, abdominal pain, heart failure or sudden death when complete heart block develops. Syncope during exertion has been reported and the disease can progress from a normal electrocardiography (ECG) to right or left bundle branch block and from the latter to complete heart block.
Lev's disease Other names Lenegre–Lev syndrome Specialty Cardiology Lev's disease is an acquired complete heart block due to idiopathic fibrosis and calcification of the electrical conduction system of the heart . Lev's disease is most commonly seen in the elderly, and is often described as senile degeneration of the conduction system. One form has been associated with SCN5A . [1] Contents 1 Presentation 1.1 Associated conditions 2 History 3 See also 4 References 5 External links Presentation [ edit ] Associated conditions [ edit ] Stokes–Adams attacks can be precipitated by this condition. These involve a temporary loss of consciousness resulting from marked slowing of the heart when the atrial impulse is no longer conducted to the ventricles. This should not be confused with the catastrophic loss of heartbeat seen with ventricular fibrillation or asystole .
A number sign (#) is used with this entry because of evidence that Brugada syndrome-5 (BRGDA5) and a nonspecific cardiac conduction defect are caused by heterozygous mutation in the SCN1B gene (600235) on chromosome 19q13. Description Brugada syndrome is characterized by an ST segment elevation in the right precordial electrocardiogram leads (so-called type 1 ECG) and a high incidence of sudden death in patients with structurally normal hearts. The syndrome typically manifests during adulthood, with a mean age of sudden death of 41 +/- 15 years, but also occurs in infants and children (summary by Antzelevitch et al., 2005). For a discussion of genetic heterogeneity of Brugada syndrome, see BRGDA1 (601144). Clinical Features Watanabe et al. (2008) studied 3 kindreds with conduction abnormalities, 1 Turkish, 1 French, and 1 Dutch; none of the families had a history of syncope, sudden cardiac death, or epilepsy.
Ten families had pure AV block, 6 had members with AV block or sinus bradycardia, and 3 had pure sinus bradycardia. ... Seven of the family members were found to have sinus node dysfunction ('sick sinus syndrome') and/or various degrees of atrioventricular block.
A number sign (#) is used with this entry because cardiac conduction defect and familial sudden death have been demonstrated to have various genetic and nongenetic causes. Variation in the AKAP10 gene (604694) has been associated with heart rate and heart rate variability, markers that predict an increased risk of sudden cardiac death. Clinical Features Green et al. (1969) described a family in which sudden death occurred in at least 10 persons in 3 generations at an average age of 21 years (range 4-44). No clinical abnormalities were detectable in members of the family, including one who died suddenly. An abnormality of the conduction system was postulated but not definitely demonstrated.
A number sign (#) is used with this entry because of evidence that progressive familial heart block type IB (PFHB1B) is caused by heterozygous mutation in the TRPM4 gene (606936) on chromosome 19q13. For a phenotypic description and a discussion of genetic heterogeneity of progressive familial heart block type I, see PFHB1A (113900). Clinical Features Brink and Torrington (1977) reported a 6-generation South African family of Portuguese and French ancestry with 261 known relatives, in which conduction defects segregated in an autosomal dominant pattern. Of 55 members in the last 3 generations who underwent electrocardiography, 31 had conduction abnormalities, including 16 with monofascicular right bundle branch block (RBBB), 3 with left anterior hemiblock, and 6 with complete heart block; another 6 individuals had a mildly prolonged QT interval or short PR interval without a Wolff-Parkinson-White (194200) pattern. The average age at which a pacemaker was implanted in the 3 successive generations decreased from 54.5 years in the fourth to 25 years in the fifth to 1 year of age in the sixth generation.
Find sources: "Chronic airway-digestive inflammatory disease" – news · newspapers · books · scholar · JSTOR ( February 2007 ) ( Learn how and when to remove this template message ) Chronic airway-digestive inflammatory disease Specialty Gastroenterology Sinus disease, allergies , and asthma have been shown to be intimately related through recent research [ citation needed ] . ... This term was first described in a book entitled Sinus Relief Now. [1] CAID directly affects the upper respiratory system (the nose and the sinuses ), the lower airway (the lungs ) and the GI tract and these areas are intimately connected. ... For example, allergies often worsen sinus problems, and sinus problems and allergies can trigger or worsen asthma . Reflux can be set off by sinus problems and reflux can also send acids up to the upper airway and worsen the inflammation already occurring secondary to infection. ... One treatment option is the so-called Five Part Plan for treatment described in the book Sinus Relief Now which includes: Using irrigation to care for sinuses, Managing the level of mould, allergens, and other pollutants in homes, offices, and cars, by cleaning up your environment Knowing which foods trigger CAID symptoms, and removing them from your diet Being compliant with your treatment.
Anomalous Aortic Origin of a Coronary Artery (AAOCA) Anomalous origin of the right coronary artery from the left coronary sinus on MRI with an inter-arterial, potentially dangerous course. Specialty Medical genetics Anomalous aortic origin of a coronary artery ( AAOCA ) is a rare congenital heart defect in which a coronary artery inappropriately arises from the aorta, usually from the incorrect sinus of Valsalva. This anomalous coronary artery often takes an interarterial (between the aorta and pulmonary artery), intraconal (within the myocardium), or intramural course (within the aortic wall), and is associated with an increased risk of sudden death in children. ... You can help by adding to it . ( February 2018 ) Treatment [ edit ] Surgical intervention is indicated for coronary artery abnormalities in symptomatic patients with AAOCA (particularly with origin of the LCA from the right sinus), such as those with serious ventricular tachyarrhythmias or documented myocardial ischemia. There are no controlled studies which have evaluated the outcome of intervention in asymptomatic individuals. [ citation needed ] The indications for intervention in asymptomatic patients with AAOCA with an intramural course are debated, especially with AAOCA RCA from the left sinus of Valsalva. Generally refer asymptomatic patients with left coronary artery arising from the right coronary sinus for surgical repair. [ citation needed ] Asymptomatic patients with the right coronary artery arising from the left sinus are managed on a case-by-case basis. ... External links [ edit ] Classification D ICD - 10 : Q24.5 ICD - 9-CM : 746.85 MeSH : D003330 DiseasesDB : 34206 External resources eMedicine : med/445 ped/2506 v t e Congenital heart defects Heart septal defect Aortopulmonary septal defect Double outlet right ventricle Taussig–Bing syndrome Transposition of the great vessels dextro levo Persistent truncus arteriosus Aortopulmonary window Atrial septal defect Sinus venosus atrial septal defect Lutembacher's syndrome Ventricular septal defect Tetralogy of Fallot Atrioventricular septal defect Ostium primum Consequences Cardiac shunt Cyanotic heart disease Eisenmenger syndrome Valvular heart disease Right pulmonary valves stenosis insufficiency absence tricuspid valves stenosis atresia Ebstein's anomaly Left aortic valves stenosis insufficiency bicuspid mitral valves stenosis regurgitation Other Underdeveloped heart chambers right left Uhl anomaly Dextrocardia Levocardia Cor triatriatum Crisscross heart Brugada syndrome Coronary artery anomaly Anomalous aortic origin of a coronary artery Ventricular inversion
This pain is usually localized to the involved sinus and may worsen when the affected person bends over or when lying down . ... Decongestants may also cause mouth dryness. [25] Once an odontogenic infection involves the maxillary sinus, it may then spread to the orbit or to the ethmoid sinus , the nasal cavity, and frontal sinuses, and in unusual instances can spread from the maxillary sinus causing orbital cellulitis , blindness, meningitis , subdural empyema , brain abscess and life-threatening cavernous sinus thrombosis. [26] [27] Infection of the eye socket is a rare complication of ethmoid sinusitis, which may result in the loss of sight and is accompanied by fever and severe illness. ... PMID 25833927 . S2CID 206469424 . ^ a b c d e f "Sinus Infection (Sinusitis)" . cdc.gov . ... Retrieved 6 April 2015 . ^ "Migraines vs. Sinus Headaches" . American Migraine Foundation . ... "Functional endoscopic balloon dilation of sinus ostia for chronic rhinosinusitis".
Find sources: "Lymphoid hyperplasia" – news · newspapers · books · scholar · JSTOR ( July 2020 ) Lymphoid hyperplasia is the rapid growth proliferation of normal cells that resemble lymph tissue. [1] Contents 1 Lymph node anatomy 2 Follicular hyperplasia 3 Paracortical hyperplasia 4 Sinus hyperplasia 5 Complications 6 See also 7 References Lymph node anatomy [ edit ] A lymph node is small, capsulated lymphoid organ that is present along the lymphatic system. ... Must be distinguished from monomorphous T cell lymphoma . Sinus hyperplasia [ edit ] Sinus hyperplasia is the preferential stimulation of the histiocytic (tissues macrophage ) compartment. Histological features include distention or engorgement of both subscapular and inatraparenchymal sinuses by benign histiocytes which may be hemo phagocytic . Sinus hyperplasia may be associated with non-hematolymphoid malignancy.