-
Hydroxyethyl Starch-Induced Pruritus
Wikipedia
Intensive Care Med . 40 (2): 160–70. doi : 10.1007/s00134-013-3156-9 . PMID 24257970 . Ständer S, Szépfalusi Z, Bohle B, Ständer H, Kraft D, Luger TA, Metze D (2001).
-
Urostealith
Wikipedia
Online version accessed on 2009-07-30. ^ S. Materazzi, R. Curini, G. D'Ascenzo, and A.
-
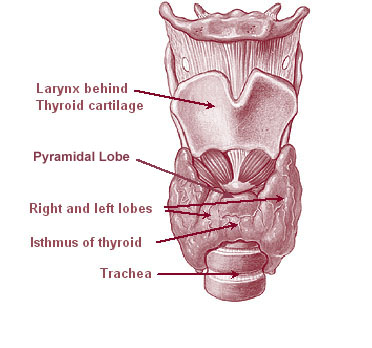
Tracheal Tumor
Wikipedia
References [ edit ] ^ Ferretti GR, Bithigoffer C, Righini CA, Arbib F, Lantuejoul S, Jankowski A (March 2009). "Imaging of tumors of the trachea and central bronchi" .
-
Cold Nodule
Wikipedia
Köln 2013, ISBN 978-3-9814660-2-7 . S. 747. ^ Fehrenbach; Herring (2012).
- Fasciitis Wikipedia
-
Warmblood Fragile Foal Syndrome
Wikipedia
References [ edit ] ^ Monthoux C, de Brot S, Jackson M, Bleul U, Walter J (January 2015).
-
Zahn Infarct
Wikipedia
. ^ Matsumoto T, Kuwabara N, Abe H, Fukuda Y, Suyama M, Fujii D, Kojima K, Futagawa S (1992), "Zahn infarct of the liver resulting from occlusive phlebitis in portal vein radicles", American Journal of Gastroenterology , 87 (3): 365–368, PMID 1539574 Reichelt HG (1985), "Partial Budd-Chiari syndrome with Zahn infarct of the liver in venous transmitted tumor thrombosis of a uterine cancer", Röntgen-Blätter (in German), 38 (11): 345–347, PMID 4081553 v t e Ischaemia and infarction Ischemia Location Brain ischemia Heart Large intestine Small intestine Infarction Types Anemic Hemorrhagic Location Heart Brain Spleen Limb Gangrene This article related to pathology is a stub .
-
Omodysplasia 2
Wikipedia
History [ edit ] This condition was first described by Maroteaux et al in 1989. [2] References [ edit ] ^ Nagasaki K, Nishimura G, Kikuchi T, Nyuzuki H, Sasaki S, Ogawa Y, Saitoh A (2018) Nonsense mutations in FZD2 cause autosomal-dominant omodysplasia: Robinow syndrome-like phenotypes.

-
Leukoencephalopathy
Wikipedia
Topics in Magnetic Resonance Imaging . 17 (4): 219–242. doi : 10.1097/RMR.0b013e31804c99d4 . PMID 17414998 . ^ Marjo S. van der Knaap and Jaap Valk, eds.CSF1R, COL4A1, TYMP, SCP2, SPP1, APP, TCN2, RHOA, MTHFR, MTR, DPYD, DARS2, BDNF, CDKN1B, NOTCH3, EIF2B2, EIF2B1, EIF2B4, CLCN2, DARS1, POLG, EIF2B5, SNORD118, RPIA, NDUFS1, NDUFAF3, HTRA1, L2HGDH, VPS11, GJC2, CLN6, TYROBP, COA8, NUBPL, EARS2, NAXE, NDUFV1, PLAA, NFE2L2, SAMHD1, NDUFS8, NDUFS6, NDUFS4, MRPS22, NDUFS3, NDUFS2, NDUFV2, TACO1, SCN8A, SCO1, YME1L1, PMPCB, AIFM1, NDUFAF1, RRM2B, TREX1, EIF2B3, NDUFB10, NDUFB11, TMEM70, FASTKD2, FOXRED1, TIMMDC1, KMT2E, NDUFAF4, TMEM126B, NDUFB9, MARS2, CTC1, PET100, AUH, NDUFS7, COX6B1, COX8A, COX10, B3GALNT2, NDUFA11, COX20, NDUFAF2, HMGCL, COX14, LAMB1, HIBCH, COLGALT1, ND2, TRNS1, ND3, NDUFAF5, NDUFA1, NDUFA6, TRNN, ND1, NDUFB3, AARS2, MLC1, EIF2S2, HEPACAM, SDHAF1, RNASET2, TUBB4A, ABCB6, LGALS14, GFAP, APOE, WARS2, CSF2, DEAF1, NFU1, PSEN1, LAMA2, KARS1, ISCA2, COA7, KCNT1, POLR3B, NOTCH2NLC, DDX59, SLC2A4RG, SHANK3, SLC26A5, GGCT, ACBD5, LYRM7, SLC5A8, RMND1, GLRX5, TREM2, MTFMT, IBA57, HIKESHI, SLC13A3, AARS1, SZT2, MS, MOG, MBP, MANBA, KIF5A, IL6, IFNG, IFNB1, HMGB1, HMBS, GJA1, GFPT1, FMR1, EIF2S3, EIF2S1, EEF1A1, EDN1, SARDH, CST3, COL4A2, CLCN1, C1QBP, ALDH3A2, ABCD1, JAG1, ADORA2A, MPV17, COX2, POLR3A, MYL2, SDS, MYL9, SCO2, FIG4, ARHGEF2, DEGS1, CUL4B, VEGFA, TUFM, TLR2, SURF1, ACTA2, SORD, SLC16A2, SLC2A1, SDHB, CCL5, PTGS2, PRPS1, PLP1, PDGFB, PAFAH1B1, NEFL, NDUFB8, NDUFA2, MTCO2P12
-
Charcot-Marie-Tooth Disease, Demyelinating, Type 1d
OMIM
INHERITANCE - Autosomal dominant NEUROLOGIC Peripheral Nervous System - Distal limb muscle weakness due to peripheral neuropathy - Distal limb muscle atrophy due to peripheral neuropathy - 'Steppage' gait - Foot drop - Decreased motor nerve conduction velocity (NCV) (less than 38 m/s) MISCELLANEOUS - Onset in first or second decade - Usually begins in feet and legs (peroneal distribution) - Upper limb involvement may occur later - Variable severity - Genetic heterogeneity (see CMT1B, 118200 ) - Allelic disorders with overlapping phenotypes include congenital hypomyelinating neuropathy (CHN, 605253 ) and Dejerine-Sottas syndrome (DSS, 145900 ) MOLECULAR BASIS - Caused by mutation in the early growth response-2 gene (EGR2, 129010.0002 ) ▲ Close
- Abruzzo–erickson Syndrome Wikipedia
-
Uremic Frost
Wikipedia
PMID 21422624 . ^ Udayakumar P, Balasubramanian S, Ramalingam KS, Lakshmi C, Srinivas CR, Mathew AC (2006).

-
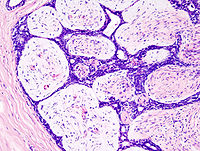
Fibroadenoma
Wikipedia
CS1 maint: DOI inactive as of December 2020 ( link ) ^ a b Pruthi S, Jones KN (February 2013). "Nonsurgical management of fibroadenoma and virginal breast hypertrophy" . Seminars in Plastic Surgery . 27 (1): 62–6. doi : 10.1055/s-0033-1343997 . PMC 3706058 . PMID 24872742 . ^ Nelson ZC, Ray RM, Wu C, Stalsberg H, Porter P, Lampe JW, Shannon J, Horner N, Li W, Wang W, Hu Y, Gao D, Thomas DB (July 2010). ... Retrieved 15 December 2007 . ^ Lim WK, Ong CK, Tan J, Thike AA, Ng CC, Rajasegaran V, Myint SS, Nagarajan S, Nasir ND, McPherson JR, Cutcutache I, Poore G, Tay ST, Ooi WS, Tan VK, Hartman M, Ong KW, Tan BK, Rozen SG, Tan PH, Tan P, Teh BT (August 2014). ... PMID 25038752 . S2CID 7623650 . ^ Piscuoglio S, Murray M, Fusco N, Marchiò C, Loo FL, Martelotto LG, Schultheis AM, Akram M, Weigelt B, Brogi E, Reis-Filho JS (November 2015). ... Seminars in Interventional Radiology . 31 (2): 193–202. doi : 10.1055/s-0034-1376159 . PMC 4078155 . PMID 25049447 . ^ a b "Management of Fibroadenomas of the Breast : Official Statement" (PDF) .MED12, RARA, TP53, ESR1, RASSF1, LOC110806263, ERBB2, WNT2, KIT, FST, LMNA, MMP2, MMP11, TP63, HMGA2, DHCR24, PRLR, TERT, UVRAG, CCL2, KHDRBS1, SCGB1D2, IGF2BP1, RB1, RHEB, EDIL3, RPE65, S100A6, CDKL1, ADAM9, VDR, CCL19, SLC5A5, TLR4, NAA10, TMPO, FOSL1, RAB40B, WNT7B, TWIST1, VEGFA, POLD3, ANXA6, CKAP4, ADAMTS8, ACVR1C, SPATA18, ADAMTS18, NUP43, MIR10A, MIR126, MIR183, MIR188, MIR21, MIR221, MIR331, MT1IP, H3P41, H3P30, H3P42, SAT2, SCIN, ADAMTS20, ANAPC7, PTEN, PRAME, CDK20, BRMS1, STEAP1, PELP1, WNT4, CENPK, ALG1, GATAD2B, MTUS1, ZNF398, ZNF410, GOLPH3, PSIP1, POLB, PSMC6, ETS1, DDX5, DNMT1, EGFR, EIF4E, FBL, ESR2, FGF1, DAXX, FGFR4, FKBP4, FLNA, MSTN, GJA1, GTF2H4, DCN, CYP17A1, HIC1, RUNX3, TRIM23, STS, CCND1, BCL2, C1QBP, CASP3, CD74, CYP1A1, CDH1, CDK4, CDKN2A, CCR5, COL5A1, CST6, HDAC2, IARS1, KLK10, MYC, MT1H, MT1JP, MT1M, MT1L, MT1X, MTNR1A, MYD88, MT1F, NF1, NFKB2, PCNA, PGR, AR, PPP1R8, MT1G, MT1E, IFNG, KRT14, IGF2, IL6, CXCR1, IL10, ING1, INHBA, LASP1, MT1B, LTB, MGMT, MMP9, MMP13, MSN, MT1A, H3P10
-
Ventriculitis
Wikipedia
ISSN 1056-9103 . S2CID 71993640 . ^ Schroeder S, Stuerenburg HJ, Escherich F, Pfeiffer G (November 2000). ... PMID 19460268 . S2CID 8371191 . ^ Muttaiyah S, Ritchie S, Upton A, Roberts S (February 2008). ... PMID 18201987 . ^ Prabhu VC, Kaufman HH, Voelker JL, Aronoff SC, Niewiadomska-Bugaj M, Mascaro S, Hobbs GR (September 1999). "Prophylactic antibiotics with intracranial pressure monitors and external ventricular drains: a review of the evidence".

-
Laryngotracheal Stenosis
Wikipedia
PMID 7742187 . ^ a b Kokturk N, Demircan S, Kurul C, Turktas H (October 2004). ... Thorac Cardiovasc Surg . 38 (1): 42–4. doi : 10.1055/s-2007-1013990 . PMID 2309228 . ^ Nouraei SA, Singh A, Patel A, Ferguson C, Howard DJ, Sandhu GS (August 2006). ... PMID 18513246 . ^ Peña J, Cicero R, Marín J, Ramírez M, Cruz S, Navarro F (October 2001). "Laryngotracheal reconstruction in subglottic stenosis: an ancient problem still present". ... PMID 14631181 . ^ Filocamo, G; Torreggiani, S; Agostoni, C; Esposito, S (April 2017).DRD1, COL2A1, SLC26A4, RSPO2, HYLS1, FRAS1, CHD7, AFF4, GRIP1, EBP, ADAMTSL2, WNT3, MAP3K7, DHCR7, RMRP, PCNT, LTBP3, KCNJ10, IDUA, HOXD13, FLNB, FLNA, FOXI1, FBN1, FREM2, TGFB1, TBX5, TBX4, CXCL8, FGF10

-
Splenomegaly
Wikipedia
Springer Science & Business Media. ISBN 9783540671367 . ^ Saboo, S S; Krajewski, K M; O'Regan, K N; Giardino, A; Brown, J R; Ramaiya, N; Jagannathan, J P (2012). ... Retrieved 20 April 2018 . ^ Ilardo, M. A.; Moltke, I.; Korneliussen, T. S.; Cheng, J.; Stern, A. J.; Racimo, F.; de Barros Damgaard, P.; Sikora, M.; Seguin-Orlando, A.; Rasmussen, S.; van den Munckhof, I. ... L.; ter Horst, R.; Joosten, L. A. B.; Netea, M. G.; Salingkat, S.; Nielsen, R.; Willerslev, E. (2018-04-18).OCLN, NRAS, HBB, PEPD, XIAP, KRAS, APOE, FAS, CYP1A2, KCNN3, STAT5B, NFE2L2, BDKRB1, FLT3, EIF2AK1, MECOM, NOTCH1, APC, AHR, MAPT, PSEN1, APP, DNASE2, TYMS, ABCB11, STX11, TNFSF11, ALMS1, TNFSF12, TNFRSF11A, ZAP70, AP3B1, GFI1B, DPM1, UROS, KLRC4, ABCA1, AP3D1, SH2B3, NPC2, AGPAT2, RNASEH2A, SEC23B, TCIRG1, RASGRP1, GNE, PLEKHM1, SLC7A7, PIEZO1, LPIN2, TTC37, SEC24C, ADAMTS3, UMPS, CLDN1, CYP7B1, TNFRSF1B, UFD1, TNFRSF4, SOX10, SMPD1, SLCO2A1, SLC4A1, SLC2A1, SKIV2L, SGSH, ATXN2, RREB1, RMRP, RHAG, RAG2, RAG1, RAB27A, PEX2, ABCD3, PTPRC, SPTA1, SPTB, AKR1D1, THPO, HIRA, TPP2, TPI1, TP53, VPS45, TNFRSF1A, TLR4, TGFB1, STAT4, TERT, TERC, TCF4, TBXAS1, TBX1, TALDO1, NEK4, KLF1, TNFRSF13B, DOLK, USB1, C15orf41, CARD11, CCDC115, ITCH, FERMT3, HSD3B7, ALPK1, CTC1, FAT4, NLRP1, CYBC1, GNPTAB, DDRGK1, VPS33A, DCLRE1C, ABCG8, ABCG5, NOD2, COX4I2, TMEM67, COG7, G6PC3, RNU4ATAC, NCF1, GPIHBP1, UBAC2, SUMF1, CAVIN1, JMJD1C, SAMD9L, IL23R, HJV, CCBE1, CDAN1, LACC1, HGSNAT, TNFRSF13C, NLRP3, PIGM, BACH2, NLRC4, HAMP, RTEL1, DCDC2, GLRX5, SBDS, FOXP3, SNX10, ICOS, OSTM1, LAT, BSCL2, SLC17A5, TINF2, IFT172, PSMB9, SF3B1, RPGRIP1L, VPS13A, NBEAL2, DYNC2LI1, ERAP1, CC2D2A, ADA2, WDR35, COG6, SCYL1, INPP5E, BTNL2, ALG1, NGLY1, NHP2, CHD7, SLC39A4, SLC30A10, NOP10, SLC29A3, STEAP3, WRAP53, MKS1, TET2, PTEN, PIK3R1, PSMB8, PSMB4, DKC1, DHCR24, DGUOK, CYBB, CYBA, CTSK, CTNS, CTLA4, CR2, CPOX, COMT, COL2A1, CCR1, CLCN7, ERCC8, LYST, CD81, DNASE1L3, EPB41, EPB42, G6PC, GLB1, GPC3, GBA, GATA2, GATA1, GALE, GAA, FUCA1, ERBB3, FOS, FMO3, FGA, GPC4, FAH, F5, ERCC6, CD40LG, SCARB2, CD28, FASLG, ATP7B, ATP6AP1, ATP6V1B2, ATM, ASAH1, ARVCF, ARSB, APOC2, B2M, APOA1, ANK1, ALDOA, ALAS2, AKT1, AGA, ADA, ATRX, CCND1, CD27, CALR, MS4A1, CD19, RUNX1, CAV1, CASR, CASP10, CASP8, CA2, BCL2, C4A, BTD, BRAF, BPGM, BMP2, BCR, BCL6, GNS, GP1BA, GP1BB, GPC1, NOTCH2, NFKB2, NFKB1, NEU1, NCF4, NCF2, NAGLU, MYD88, MVK, MMUT, MST1, MPL, MIF, MEFV, MCM4, MAN2B1, LYZ, PNP, OTC, PARN, PIK3CD, PSAP, PRKCD, PRF1, PPARG, PKHD1, PKLR, ABL1, PIK3CA, PDGFRA, PIK3C2A, PHYH, PHKG2, PHKA2, ABCB4, ATP8B1, PEX7, SH2D1A, LPL, IGH, HFE, IDUA, IDS, IRF8, HPGD, HLA-DRB1, HLA-B, HK1, HBG2, LMNA, HBG1, HBA2, HBA1, GYPC, GUSB, GPR35, GPI, IFNGR1, IL12A-AS1, IL1RN, IL2RA, LIPA, LIG4, LCAT, LBR, KCNN4, KCNH1, JAK2, ITK, INPPL1, IL12A, IL10, IL7R, IL6, IL2RG, IL2RB, HLA-DQB1, VEGFA, TNFRSF8

-
Anemia Of Prematurity
Wikipedia
PMID 10920175 . ^ Adams, M., Benitz, W., Geaghan, S., Kumar, R., Madan, A., & Widness, J. (2005). ... Retrieved December 9, 2007, from EbscoHost Research Databases. ^ a b Brown, Mark S.; Keith, Julian F. (1999-08-01). "Comparison Between Two and Five Doses a Week of Recombinant Human Erythropoietin for Anemia of Prematurity: A Randomized Trial". ... S2CID 24961879 . ^ Bain, A., & Blackburn, S. (2004). Issues in transfusing preterm infants in the NICU. ... S2CID 21928067 . ^ New, H. V.; Stanworth, S. J.; Engelfriet, C. P.; Reesink, H. ... K.; Savoia, H. F.; Wood, E. M.; Olyntho, S.; Trigo, F. (2009). "Neonatal transfusions".
-
Mesoblastic Nephroma
Wikipedia
Among patients with these risk factors, only those with lymph node involvement are recommended for further therapy. [4] It has been suggested that mesoblastic nephroma patients with lymph node involvement or recurrent disease might benefit by adding the ALK inhibitor , crizotinib , or a tyrosine kinase inhibitor, either larotrectinib or entrectinib , to surgical, radiation, and/or chemotherapy treatment regimens. These drugs inhibit NTRK3's tyrosine kinase activity. [1] Crizotinib has proven useful in treating certain cases of acute lymphoblastic leukemia that are associated with the ETV6-NTRK3 fusion gene while larotrectinib and entrectinib have been useful in treating various cancers (e.g. a metastatic sarcoma , papillary thyroid cancer , non-small-cell lung carcinoma , gastrointestinal stromal tumor , mammary analog secretory carcinoma , and colorectal cancer ) that are driven by mutated, overly active tyrosine kinases. ... PMID 27020209 . ^ a b c d e Wang ZP, Li K, Dong KR, Xiao XM, Zheng S (2014). "Congenital mesoblastic nephroma: Clinical analysis of eight cases and a review of the literature" . ... PMID 24066765 . ^ Anderson J, Gibson S, Sebire NJ (2006). "Expression of ETV6-NTRK in classical, cellular and mixed subtypes of congenital mesoblastic nephroma". ... European Journal of Cancer . 48 (14): 2219–26. doi : 10.1016/j.ejca.2012.04.009 . PMID 22579455 . ^ Alavi S, Khoddami M, Yazdi MK, Dehghanian P, Esteghamati S (2013).
-
Hysteria
Wikipedia
Augustine's writings suggested that human suffering resulted from sin, and thus, hysteria became perceived as satanic possession. [6] With the shift in perception of hysteria came a shift in treatment options. [6] Instead of admitting patients to a hospital, the church began treating patients through prayers, amulets, and exorcisms . [6] Furthermore, during the medieval and Renaissance periods many patients of hysteria were prosecuted as witches and underwent interrogations, torture, and execution. [6] However, during the sixteenth and seventeenth centuries activists and scholars worked to change the perception of hysteria back to a medical condition. [3] Particularly, French physician Charles Lepois insisted that hysteria was a malady of the brain. [7] In addition, in 1697, English physician Thomas Sydenham theorized that hysteria was an emotional condition, instead of a physical condition. [3] Many physicians followed Lepois and Sydenham's lead and hysteria became disassociated with the soul and the womb. [7] During this time period science started to focalize hysteria in the central nervous system. [7] As doctors developed a greater understanding of the human nervous system, the neurological model of hysteria was created, which further propelled the conception of hysteria as a mental disorder. [7] In 1859, Paul Briquet defined hysteria as a chronic syndrome manifesting in many unexplained symptoms throughout the body's organ systems. [8] What Briquet described became known as Briquet's syndrome, or Somatization disorders , in 1971. [9] Over a ten year period, Briquet conducted 430 case studies of patients with hysteria. [8] Following Briquet, Jean-Martin Charcot studied women in an asylum in France and used hypnosis as treatment. [3] He also mentored Pierre Janet , another French psychologist, who studied five of hysteria's symptoms (anesthesia, amnesia, abulia, motor control diseases, and character change) in depth and proposed that hysteria symptoms occurred due to a lapse in consciousness. [10] Both Charcot and Janet inspired Sigmund Freud 's work. [11] Freud theorized hysteria stemmed from childhood sexual abuse or repression, and was also one of the first to apply hysteria to men. [11] During the 20th century, as psychiatry advanced in the West, anxiety and depression diagnoses began to replace hysteria diagnoses in Western countries. [3] For example, from 1949 to 1978, annual admissions of hysteria patients in England and Wales decreased by roughly two thirds. [3] With the decrease of hysteria patients in Western cultures came an increase in anxiety and depression patients. [3] Although declining in the West, in Eastern countries such as Sudan, Egypt, and Lebanon hysteria diagnoses remained consistent. [3] Theories for why hysteria diagnoses began to decline vary, but many historians infer that World War II, westernization, and migration shifted Western mental health expectations. [3] [11] Twentieth century western societies expected depression and anxiety manifest itself more in post World War II generations and displaced individuals; and thus, individuals reported or were diagnosed accordingly. [3] In addition, medical advancements explained ailments that were previously attributed to hysteria such as epilepsy or infertility. [9] In 1980, after a gradual decline in diagnoses and reports, hysteria was removed from the American Psychiatric Association 's Diagnostic and Statistical Manual of Mental Disorders (DSM), which had included hysteria as a mental disorder from its second publication in 1968. [9] Historical symptoms [ edit ] Historically, the symptoms of hysteria have a large range. [12] [13] [10] Hysteria Patient For example: Shortness of breath Anxiety Insomnia Fainting Amnesia Paralysis Pain Spasms Convulsive fits Vomiting Deafness Bizarre movements Seizures Hallucinations Inability to speak [12] [13] [10] Notable figures [ edit ] Jean-Martin Charcot [ edit ] In the late nineteenth century, French neurologist Jean-Martin Charcot , attempted to tackle what he referred to as, "the great neurosis" or hysteria. [14] Charcot theorized that hysteria was a hereditary, physiological disorder. [14] He believed hysteria impaired areas of the brain which provoked the physical symptoms displayed in each patient. [14] While Charcot believed hysteria was hereditary, he also thought that environmental factors such as stress could trigger hysteria in an individual. [15] Charcot published over 120 case studies of patients who he diagnosed with hysteria, including Marie "Blanche" Whittman. [16] Whittman was referred to as the "Queen of Hysterics," and remains the most famous patient of hysteria. [16] To treat his patients, Charcot used hypnosis, which he determined was only successful when used on hysterics. [16] Using patients as props, Charcot executed dramatic public demonstrations of hysterical patients and his cures for hysteria, which many suggest produced the hysterical phenomenon. [16] Furthermore, Charcot noted similarities between demon possession and hysteria, and thus, he concluded "demonomania" was a form of hysteria. [3] Sigmund Freud [ edit ] In 1896, Sigmund Freud , who was an Austrian psychiatrist, published " The Aetiology of Hysteria ". [17] The paper explains how Freud believes his female patients' neurosis, which he labels hysteria, resulted from sexual abuse as children. [17] Freud named the concept of physical symptoms resulting from childhood trauma: hysterical conversion. [17] Freud hypothesized that in order to cure hysteria the patient must relive the experiences through imagination in the most vivid form while under light hypnosis . [17] However, Freud later changed his theory. [17] His new theory claimed that his patients imagined the instances of sexual abuse, which were instead repressed childhood fantasies. [17] By 1905, Freud retracted the theory of hysteria resulting from repressed childhood fantasies. ... ISBN 9781785927416 . ^ a b c d e f g h i j k North, Carol S. (November 6, 2015). "The Classification of Hysteria and Related Disorders: Historical and Phenomenological Considerations" . ... PMID 26561836 . ^ a b c d e f g h i j k l m n o Micale, Mark S. (January 15, 2019). Approaching Hysteria: Disease and Its Interpretations . ... ISBN 978-1-4832-2166-3 . ^ a b c d Gilman, Sander Lawrence; Gilman, Sander L.; King, Helen; Porter, Roy; Rousseau, G. S.; Showalter, Elaine (January 1, 1993).

-
Anorgasmia
Wikipedia
. ^ http://www.atforum.com/pdf/europad/HeroinAdd6-3.pdf ^ Bridley, G. S.; Gillan, P. (1982). "Men and women who do not have orgasms". ... Retrieved 6 December 2011 . ^ Humphery, S.; Nazareth, I. (1 October 2001). "GPs' views on their management of sexual dysfunction" . ... PMID 11604374 . ^ Brotto LA, Bitzer J, Laan E, Leiblum S, Luria M (2010). "Women's Sexual Desire and Arousal Disorders". ... PMID 17486282 . ^ Shrivastava RK, Shrivastava S, Overweg N, Schmitt M (1995). "Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors". Journal of Clinical Psychopharmacology . 15 (1): 83–84. doi : 10.1097/00004714-199502000-00014 . PMID 7714234 . ^ Balogh S, Hendricks SE, Kang J (1992). "Treatment of fluoxetine-induced anorgasmia with amantadine".








