Amplitudes can vary significantly with tool design, condition and style of use, even for the same type of tool. [ citation needed ] In the UK, Health and Safety Executive gives the example of a hammer drill which can vary from 6 m/s² to 25 m/s². HSE publishes a list of typically observed vibration levels for various tools, and graphs of how long each day a worker can be exposed to particular vibration levels.
. ^ Fernández O.; Fernández V.E.; Guerrero M. (2015). "Demyelinating diseases of the central nervous system". Medicine . 11 (77): 4601–4609. doi : 10.1016/j.med.2015.04.001 . ^ Poser C. M. (1961). "Leukodystrophy and the Concept of Dysmyelination".
The disorder seems to begin rarely in early infancy. However, the paucity of myelin in the cerebral hemispheres during the first 4 to 6 months of life would make histopathologic classification on the basis of myelin breakdown difficult at this stage. Progression is usually subacute in pace. Cortical blindness is often a conspicuous feature. Sibs may show great differences in the site of the lesion, age of onset, and rate of progression (Meyer and Pilkington, 1936). All cases reported as familial Schilder disease are probably in fact sudanophilic cerebral sclerosis, Krabbe disease (245200), or metachromatic leukoencephalopathy (250100). If the term is to be preserved at all, its use should be confined to sudanophilic cerebral sclerosis.
Schilder's disease is a progressive demyelinating disorder of the central nervous system. Epidemiology Less than 20 sporadic cases (predominantly males) have been reported so far. Clinical description The onset is usually in childhood (age 5-14 years). The disease often occurs shortly after an infectious illness and may manifest with headache, malaise and fever. Variable neurological abnormalities progressively develop and include personality changes, poor attention, dementia, aphasia, headache, vomiting, tremor, seizures, balance instability, incontinence, muscle weakness.
For the autosomal recessive, neonatal onset disease, see Neonatal adrenoleukodystrophy . Adrenoleukodystrophy Other names X-linked adrenoleukodystrophy, ALD, X-ALD, Siemerling–Creutzfeldt disease, bronze Schilder disease White matter , with reduced volume and increased signal intensity. The anterior white matter is spared. Features are consistent with X-linked adrenoleukodystrophy. Pronunciation /- ˌ lj uː k oʊ ˈ d ɪ s t r ə f i / Specialty Medical genetics Types X-Linked ALD Adrenoleukodystrophy (ALD) is a disease linked to the X chromosome . It is a result of fatty acid buildup caused by a defect in the very long chain of fatty acids transporter in peroxisomes, which then causes damage to the myelin sheath of the nerves , resulting in seizures and hyperactivity.
Springer. p. 336. ISBN 9783319608143 . ^ Rabiu M, Alhassan MB, Ejere HO, Evans JR (2012). ... Veterinary Ophthalmology . 12 (4): 221–226. doi : 10.1111/j.1463-5224.2009.00705.x . PMID 19604337 . ^ Bojrab, M Joseph (1998). Current techniques in small animal surgery .
Overview Entropion (en-TROH-pee-on) is a condition in which your eyelid turns inward so that your eyelashes and skin rub against the eye surface. This causes irritation and discomfort. When you have entropion, your eyelid may be turned in all the time or only when you blink hard or squeeze your eyelids shut. Entropion is more common in older adults, and it generally affects only the lower eyelid. Artificial tears and lubricating ointments can help relieve symptoms of entropion. But usually surgery is needed to fully correct the condition. Left untreated, entropion can cause damage to the transparent covering in the front part of your eye (cornea), eye infections and vision loss.
See also [ edit ] Hypertensive crisis List of systemic diseases with ocular manifestations Ophthalmology Optometry References [ edit ] ^ a b Bhargava, M; Ikram, M K; Wong, T Y (2011). "How does hypertension affect your eyes?"
A number sign (#) is used with this entry because argininosuccinic aciduria is caused by homozygous mutation in the gene encoding argininosuccinate lyase (ASL; 608310) on chromosome 7q11. Description Argininosuccinic aciduria is an autosomal recessive disorder of the urea cycle. Urea cycle disorders are characterized by the triad of hyperammonemia, encephalopathy, and respiratory alkalosis. Five disorders involving different defects in the biosynthesis of the enzymes of the urea cycle have been described: ornithine transcarbamylase deficiency (311250), carbamyl phosphate synthetase deficiency (237300), argininosuccinate synthetase deficiency, or citrullinemia (215700), argininosuccinate lyase deficiency, and arginase deficiency (207800). Erez (2013) reviewed argininosuccinic aciduria and progress in understanding it as a monogenic disorder that, like other inborn errors of metabolism, manifests as a multifactorial disorder at the phenotypic level.
Arginine base supplementation The doses of arginine base routinely recommended are 400-700 mg/kg/day in persons weighing ˂20 kg & 8.8-15.4 g/m 2 /day in those weighing >20 kg. The authors prefer to use a lower dose of arginine whenever possible, in the range of 100-250 mg/kg/day. ... Oral nitrogen-scavenging therapy (an alternative pathway therapy in which sodium benzoate & phenyl butyrate stimulate the excretion of nitrogen in the form of hippuric acid & phenylacety-lglutamine, respectively) The typical dose ranges 2 for the medications: Sodium phenylbutyrate, 400-600 mg/kg/day for persons weighing ≤20 kg; 9.9-13 g/m 2 /day for those weighing >20 kg Glycerol phenylbutyrate, 4.4-11.2 mL/m 2 /day Sodium benzoate, 250-500 mg/kg/day or 5.5 g/m 2 /day Individuals who have had frequent metabolic decompensations or episodes of ↑ ammonia despite being on a protein-restricted diet & arginine base supplementation are candidates for oral nitrogen-scavenging therapy.
Argininosuccinic aciduria is an inherited disorder that causes ammonia to accumulate in the blood. Ammonia, which is formed when proteins are broken down in the body, is toxic if the levels become too high. The nervous system is especially sensitive to the effects of excess ammonia. Argininosuccinic aciduria usually becomes evident in the first few days of life. An infant with argininosuccinic aciduria may be lacking in energy (lethargic) or unwilling to eat, and have poorly controlled breathing rate or body temperature.
A rare, genetic disorder of urea cycle metabolism typically characterized by either a severe, neonatal-onset form that manifests with hyperammonemia accompanied with vomiting, hypothermia, lethargy and poor feeding in the first few days of life, or late-onset forms that manifest with stress- or infection-induced episodic hyperammonemia or, in some, behavioral abnormalities and/or learning disabilities, or chronic liver disease. Patients often manifest liver dysfunction. Epidemiology The prevalence at birth of argininosuccinic aciduria (ASA) ranges between 1/70,000-218,000 worldwide. Clinical description ASA can have a variable clinical picture with either a neonatal-onset or a late-onset (at any age outside the newborn period). Neonates with severe neonatal-onset ASA usually appear normal during the first 24-48 hours after birth but within a few days present with severe hyperammonemia manifesting with lethargy, somnolence, refusal to feed, vomiting, tachypnea and respiratory alkalosis. If untreated, worsening lethargy, seizures, coma and death may occur.
Argininosuccinic aciduria is an inherited disorder that causes ammonia to accumulate in the blood. Ammonia, which is formed when proteins are broken down in the body, is toxic if the levels become too high. The nervous system is especially sensitive to the effects of excess ammonia. Argininosuccinic aciduria usually becomes evident in the first few days of life. An infant with argininosuccinic aciduria may be lacking in energy (lethargic) or unwilling to eat, and have a poorly controlled breathing rate or body temperature.
. ^ Costache, Mădălina Elena; Frick, Andreas; Månsson, Kristoffer; Engman, Jonas; Faria, Vanda; Hjorth, Olof; Hoppe, Johanna M.; Gingnell, Malin; Frans, Örjan; Björkstrand, Johannes; Rosén, Jörgen (29 April 2020). ... Archived from the original (PDF) on 24 April 2016. ^ Hassall, Trevor; Arquero, Jose L.; Joyce, John; Gonzalez, Jose M. (12 July 2013). "Communication apprehension and communication self‐efficacy in accounting students" (PDF) .
PMC 5602357 . PMID 28814376 . ^ Weinreich, M; Yu, PJ; Trost, B (2015). "Sinus of valsalva aneurysms: review of the literature and an update on management" . ... PMID 28814376 . ^ Kenny, Damien; Hijazi, Ziyad M. (December 2011). "Transcatheter approaches to non-valvar structural heart disease".
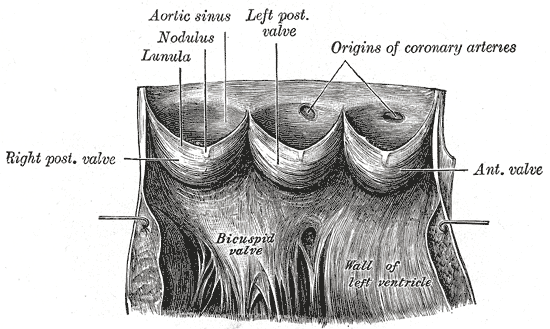
Sinus of Valsalva aneurysm (SVA) is a rare congenital heart malformation of one or more of the aortic sinuses, consisting of a dilation that when unruptured is usually asymptomatic but when ruptured presents with progressive exertional dyspnea, fatigue, chest pain and that can lead to congestive heart failure if left untreated.
., Marchiori, P. E. R., Cantarella, H., & Landell, M. G. A. (2014). Sugarcane performance under phosphorus deficiency: physiological responses and genotypic variation. ... L., Schepers, J. S., Francis, D. D., & Schlemmer, M. R. (2002). Detection of Phosphorus and Nitrogen Deficiencies in Corn Using Spectral Radiance Measurements.
Cementoblastoma Specialty Dentistry Cementoblastoma , or benign cementoblastoma , is a relatively rare benign neoplasm of the cementum of the teeth . It is derived from ectomesenchyme of odontogenic origin. [1] Less than 0.69–8% of all tumors of the teeth.there is no paresthesia. Contents 1 Signs and symptoms 2 Diagnosis 3 Treatment 4 See also 5 References 6 External links Signs and symptoms [ edit ] Cementoblastoma usually occurs in people under the age of 25, particularly males. It usually involves the permanent mandibular molars or premolars. [2] The involved tooth usually has a vital pulp . It is attached to the tooth root and may cause its resorption, may involve the pulp canal , grows slowly, tends to expand the overlying cortical plates, and, except for the enlargement produced, is usually asymptomatic.
It is hypothesized, based on CT scanning, that of the two sexes experiencing post-stroke depression, women who had post-stroke depression had a higher rate of left hemisphere lesions than men. [5] However, risk of post-stroke depression can not be determined effectively based on the location of the lesion in the brain and more research in this area is needed. [6] It has also been postulated that the risk of developing post-stroke depression in male patients is partly linked to having a high level of limitations and disability in functioning, especially in performing activities of daily living (ADL's), as a result of their stroke; the greater the limitation, the greater the severity. [5] Risk of developing depression post-stroke in women is partly linked to a history of psychological disorders as well as limitations involving cognition as a result of their stroke. [5] References [ edit ] ^ Miller, Jeffrey M.; Vorel, Stanislav R.; Tranguch, Anthony J.; Kenny, Edward T.; Mazzoni, Pietro; van Gorp, Wilfred G.; Kleber, Herbert D. ... PMID 9547465 . ^ Carson, Alan J.; MacHale, Siobhan; Allen, Kathryn; Lawrie, Stephen M.; Dennis, Martin; House, Allan; Sharpe, Michael (8 July 2000).
.; Zalewski, Adam; Dick, Bernhard; Frey, Brigitte M.; Monné, Raquel; Torán, Núria; Audí, Laura (29 April 2018). ... T.; Koper, Jan W.; Boehmer, Annemie L. M.; Themmen, Axel P. N.; Verhoef-Post, Miriam; Timmerman, Marianna A.; Otten, Barto J.; Drop, Stenvert L.
. ^ a b c Schankin, CJ, Maniyar, FH, Sprenger, T, Chou, DE, Eller, M, Goadsby, PJ, 2014, The Relation Between Migraine, Typical Migraine Aura and "Visual Snow", Headache, doi : 10.1111/head.12378 ^ a b Raghavan, Manoj; Remler, Bernd F.; Rozman1, Stephanie; Pelli, Denis G. (2010). ... PMID 16837189 . ^ Podoll K, Dahlem M, Greene S. Persistent migraine aura symptoms aka visual snow.
Washington, DC: Armed Forces Institute of Pathology, 1994; 101–135. ^ a b c d e f Chung, Ellen M.; Specht, Charles S.; Schroeder, Jason W. ... American Journal of Ophthalmology . 133 (6): 841–843. doi : 10.1016/S0002-9394(02)01432-0 . ^ Janss, Anna J.; Yachnis, Anthony T.; Silber, Jeffrey H.; Trojanowski, John Q.; Lee, Virginia M.-Y.; Sutton, Leslie N.; Perilongo, Giorgio; Rorke, Lucy B.; Phillips, Peter C.
Medulloepithelioma of the central nervous system is a rare, primitive neuroectodermal tumor characterized by papillary, tubular and trabecular arrangements of neoplastic neuroepithelium, mimicking the embryonic neural tube, most commonly found in the periventricular region within the cerebral hemispheres, but has also been reported in brainstem and cerebellum. It usually presents in childhood with headache, nausea, vomiting, facial nerve paresis, and/or cerebellar ataxia, and typically has a progressive course, highly malignant behavior and poor prognosis. Hearing and visual loss have also been observed.
Medulloepithelioma Histopathology of medulloepithelioma showing characteristic neural tube like strands. Specialty Neurosurgery , oncology Medulloepithelioma is a rare, primitive, fast-growing brain tumour thought to stem from cells of the embryonic medullary cavity . [1] Tumours originating in the ciliary body of the eye are referred to as embryonal medulloepitheliomas, [1] or diktyomas . [2] A highly malignant undifferentiated primitive neuroepithelial tumour of children, medulloepithelioma may contain bone , cartilage , skeletal muscle , and tends to metastasize extracranially. [2] Contents 1 Signs and symptoms 2 Diagnosis 2.1 Classification 3 Treatment 4 Prognosis 5 Epidemiology 6 References 7 External links Signs and symptoms [ edit ] Medulloepithelioma have been reported to occur in the cerebral hemispheres , brainstem , cerebellum , and peripheral sites . [3] [4] [5] [6] Due to rapid growth of the tumour, patients typically present with increased intracranial pressure , seizures , and focal neurologic signs . [7] Diagnosis [ edit ] Neuronal differentiation, ranging from neuroblasts to ganglion cells, is seen in some medulloepitheliomas. Imaging studies such as Computerized Tomography (CT) and Magnetic Resonance Imaging (MRI) can aid diagnosis . Medulloepithelioma appears isodense or hypodense with variable heterogeneity and calcification on non-contrast CT scan, and enhances with contrast. [3] This radiographical finding is consistent with a primitive neuroectodermal tumour, especially in children. [6] Blood studies and imaging studies of the abdomen may be used to detect metastases. [6] Needle aspiration biopsy can be used to aid diagnosis. [6] Definitive diagnosis requires histopathological examination of surgically excised tumour tissues. Histologically, medulloepithelioma resemble a primitive neural tube and with neuronal, glial and mesenchymal elements. [8] [9] Flexner-Wintersteiner rosettes may also be observed. [10] Immunohistochemically , neural tube-like structures are vimentin positive in the majority of medulloepitheliomas. [11] Poorly differentiated medulloepitheliomas are vimentin negative.
.; Nakamura, K.; Akune, T.; Yoshida, M. (2012). "Prevalence of symptomatic lumbar spinal stenosis and its association with physical performance in a population-based cohort in Japan: theWakayama Spine Study" (PDF) . ... ISSN 0028-4793 . PMID 18287604 . ^ Fletcher, Jack M.; Brei, Timothy J. (2010-01-01). "Introduction: Spina bifida—A multidisciplinary perspective" .
This article needs more medical references for verification or relies too heavily on primary sources . Please review the contents of the article and add the appropriate references if you can. Unsourced or poorly sourced material may be challenged and removed . Find sources: "Spondylopathy" – news · newspapers · books · scholar · JSTOR ( June 2019 ) Spondylopathy Specialty Rheumatology Spondylopathies are disorders of the vertebrae . When involving inflammation , it can be called spondylitis . In contrast, a spondyloarthropathy is a condition involving the vertebral joints , but many conditions involve both spondylopathy and spondyloarthropathy. Examples include ankylosing spondylitis and spondylosis . See also [ edit ] Dorsopathies Spondyloarthropathy Spondylolisthesis Spondylosis Spondylitis Spondylolysis References [ edit ] External links [ edit ] Classification D ICD - 10 : M45 - M49 ICD - 9-CM : 720 - 724 v t e Spinal disease Deforming Spinal curvature Kyphosis Lordosis Scoliosis Other Scheuermann's disease Torticollis Spondylopathy inflammatory Spondylitis Ankylosing spondylitis Sacroiliitis Discitis Spondylodiscitis Pott disease non inflammatory Spondylosis Spondylolysis Spondylolisthesis Retrolisthesis Spinal stenosis Facet syndrome Back pain Neck pain Upper back pain Low back pain Coccydynia Sciatica Radiculopathy Intervertebral disc disorder Schmorl's nodes Degenerative disc disease Spinal disc herniation Facet joint arthrosis This article about a disease of musculoskeletal and connective tissue is a stub .
. ^ a b Gnepp DR, Wang LJ, Brandwein-Gensler M, et al. (Feb 2006). "Sclerosing polycystic adenosis of the salivary gland: a report of 16 cases". ... PMID 16434888 . ^ Skalova A, Michal M, Simpson RH, et al. (Jan 2002). "Sclerosing polycystic adenosis of parotid gland with dysplasia and ductal carcinoma in situ.
A recent study distinguishes between mild and severe polyhydramnios and showed that Apgar score of less than 7, perinatal death and structural malformations only occurred in women with severe polyhydramnios. [6] In another study, all patients with polyhydramnios, that had a sonographically normal fetus, showed no chromosomal anomalies. [4] (M/C for polyhydramnio is fetal anomalies 'Williams Obstetrics, 24th Edition – Cunningham, Leveno, Bloom et al. ... CS1 maint: multiple names: authors list ( link ) ^ Bundgaard A, Andersen BR, Rode L, Lebech M, Tabor A, Prevalence of polyhydramnios at a Danish hospital—a population-based study.
Overview Polyhydramnios (pol-e-hi-DRAM-nee-os) is the excessive accumulation of amniotic fluid — the fluid that surrounds the baby in the uterus during pregnancy. Polyhydramnios occurs in about 1 to 2 percent of pregnancies. Most cases of polyhydramnios are mild and result from a gradual buildup of amniotic fluid during the second half of pregnancy. Severe polyhydramnios may cause shortness of breath, preterm labor, or other signs and symptoms. If you're diagnosed with polyhydramnios, your health care provider will carefully monitor your pregnancy to help prevent complications. Treatment depends on the severity of the condition. Mild polyhydramnios may go away on its own.
It was later described in the United States after vaccinating horses for Eastern Equine Encephalitis , again using live virus vaccines and equine-derived antiserum. [1] It has since been reported throughout North America and Europe. [2] References [ edit ] ^ a b c d e f g h i j k Reed, Stephen M., Waewick M. Bayly, and Debra C. Sellon. (2010).