Chronic Obstructive Pulmonary Disease

Chronic obstructive pulmonary disease (COPD) is a type of obstructive lung disease characterized by long-term breathing problems and poor airflow. The main symptoms include shortness of breath and cough with sputum production. COPD is a progressive disease, meaning it typically worsens over time. Eventually, everyday activities such as walking or getting dressed become difficult. Chronic bronchitis and emphysema are older terms used for different types of COPD. The term "chronic bronchitis" is still used to define a productive cough that is present for at least three months each year for two years. Those with such a cough are at a greater risk of developing COPD. The term "emphysema" is also used for the abnormal presence of air or other gas within tissues.
The most common cause of COPD is tobacco smoking, with a smaller number of cases due to factors such as air pollution and genetics. In the developing world, common sources of air pollution are wood combustion and cooking fires. Long-term exposure to these irritants causes an inflammatory response in the lungs, resulting in narrowing of the small airways and breakdown of lung tissue. The diagnosis is based on poor airflow as measured by lung function tests. In contrast to asthma, the airflow reduction generally does not improve much with the use of a bronchodilator.
Most cases of COPD can be prevented by reducing exposure to risk factors. This includes decreasing rates of smoking and improving indoor and outdoor air quality. While treatment can slow worsening, no cure is known. COPD treatments include smoking cessation, vaccinations, respiratory rehabilitation, and often inhaled bronchodilators and steroids. Some people may benefit from long-term oxygen therapy or lung transplantation. In those who have periods of acute worsening, increased use of medications, antibiotics, steroids, and hospitalization may be needed.
As of 2015, COPD affected about 174.5 million people (2.4% of the global population). It typically occurs in people over the age of 40. Males and females are affected equally commonly. In 2015, it caused 3.2 million deaths, more than 90% in the developing world, up from 2.4 million deaths in 1990. The number of deaths is projected to increase further because of higher smoking rates in the developing world, and an ageing population in many countries. It resulted in an estimated economic cost of US$2.1 trillion in 2010.
Signs and symptoms
 87/Gnome-mime-sound-openclipart.svg/50px-Gnome-mime-sound-openclipart.svg.png" decoding="async" width="50" height="50" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/8/
87/Gnome-mime-sound-openclipart.svg/50px-Gnome-mime-sound-openclipart.svg.png" decoding="async" width="50" height="50" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/8/The most common symptoms of COPD are shortness of breath, and a cough that produces sputum. These symptoms are present for a prolonged period of time and typically worsen over time. It is unclear whether different types of COPD exist. While previously divided into emphysema and chronic bronchitis, emphysema is only a description of lung changes rather than a disease itself, and chronic bronchitis is simply a descriptor of symptoms that may or may not occur with COPD.
Cough
A chronic cough is often the first symptom to develop. Early on it may just occur occasionally or may not result in sputum. When a cough persists for more than three months each year for at least two years, in combination with sputum production and without another explanation, it is by definition chronic bronchitis. Chronic bronchitis can occur before the restricted airflow and thus COPD fully develops. The amount of sputum produced can change over hours to days. In some cases, the cough may not be present or may only occur occasionally and may not be productive. Some people with COPD attribute the symptoms to a "smoker's cough". Sputum may be swallowed or spat out, depending often on social and cultural factors. In severe COPD, vigorous coughing may lead to rib fractures or to a brief loss of consciousness. Those with COPD often have a history of "common colds" that last a long time.
Shortness of breath
Shortness of breath is a common symptom and is often the most distressing. It is commonly described as: "my breathing requires effort," "I feel out of breath," or "I can't get enough air in." Different terms, however, may be used in different cultures. Typically, the shortness of breath is worse on exertion of a prolonged duration and worsens over time. In the advanced stages, or end stage pulmonary disease, it occurs during rest and may be always present. Shortness of breath is a source of both anxiety and a poor quality of life in those with COPD. Many people with more advanced COPD breathe through pursed lips and this action can improve shortness of breath in some.
Physical activity limitation
COPD often leads to reduction in physical activity, in part due to shortness of breath. In later stages of COPD muscle wasting (cachexia) may occur. Low levels of physical activity are associated with worse outcomes.
Other symptoms
In COPD, breathing out may take longer than breathing in. Chest tightness may occur, but is not common and may be caused by another problem. Those with obstructed airflow may have wheezing or decreased sounds with air entry on examination of the chest with a stethoscope. A barrel chest is a characteristic sign of COPD, but is relatively uncommon. Tripod positioning may occur as the disease worsens.
Advanced COPD leads to high pressure on the lung arteries, which strains the right ventricle of the heart. This situation is referred to as cor pulmonale, and leads to symptoms of leg swelling and bulging neck veins. COPD is more common than any other lung disease as a cause of cor pulmonale. Cor pulmonale has become less common since the use of supplemental oxygen.
COPD often occurs along with a number of other conditions, due in part to shared risk factors. These conditions include ischemic heart disease, high blood pressure, diabetes mellitus, muscle wasting, osteoporosis, lung cancer, anxiety disorder, sexual dysfunction, and depression. In those with severe disease, a feeling of always being tired is common. Fingernail clubbing is not specific to COPD and should prompt investigations for an underlying lung cancer.
Exacerbation
An acute exacerbation of COPD is defined as increased shortness of breath, increased sputum production, a change in the color of the sputum from clear to green or yellow, or an increase in cough in someone with COPD. They may present with signs of increased work of breathing such as fast breathing, a fast heart rate, sweating, active use of muscles in the neck, a bluish tinge to the skin, and confusion or combative behavior in very severe exacerbations. Crackles may also be heard over the lungs on examination with a stethoscope.
Cause
The primary cause of COPD is tobacco smoke, with occupational exposure and pollution from indoor fires being significant causes in some countries. Typically, these must occur over several decades before symptoms develop. A person's genetic makeup also affects the risk.
Smoking


The primary risk factor for COPD globally is tobacco smoking. Of those who smoke, about 20% will get COPD, and of those who are lifelong smokers, about half will get COPD. In the United States and United Kingdom, of those with COPD, 80–95% are either current or previous smokers. The likelihood of developing COPD increases with the total smoke exposure. Additionally, women are more susceptible to the harmful effects of smoke than men. In non-smokers, exposure to second-hand smoke is the cause in up to 20% of cases. Other types of smoke, such as, marijuana, cigar, and water-pipe smoke, also confer a risk. Water-pipe smoke appears to be as harmful as smoking cigarettes. Problems from marijuana smoke may only be with heavy use. Women who smoke during pregnancy may increase the risk of COPD in their child. For the same amount of cigarette smoking, women have a higher risk of COPD than men.
Air pollution

Poorly ventilated cooking fires, often fueled by coal or biomass fuels such as wood and dung, lead to indoor air pollution and are one of the most common causes of COPD in developing countries. These fires are a method of cooking and heating for nearly 3 billion people, with their health effects being greater among women due to greater exposure. They are used as the main source of energy in 80% of homes in India, China and sub-Saharan Africa.
People who live in large cities have a higher rate of COPD compared to people who live in rural areas. While urban air pollution is a contributing factor in exacerbations, its overall role as a cause of COPD is unclear. Areas with poor outdoor air quality, including that from exhaust gas, generally have higher rates of COPD. The overall effect in relation to smoking, however, is believed to be small.
Occupational exposure
Intense and prolonged exposure to workplace dusts, chemicals, and fumes increases the risk of COPD in both smokers and nonsmokers. Workplace exposure is believed to be the cause in 10–20% of cases. In the United States, it is believed that it is related to more than 30% of cases among those who have never smoked and probably represents a greater risk in countries without sufficient regulations.
A number of industries and sources have been implicated, including high levels of dust in coal mining, gold mining, and the cotton textile industry, occupations involving cadmium and isocyanates, and fumes from welding. Working in agriculture is also a risk. In some professions, the risks have been estimated as equivalent to that of one-half to two packs of cigarettes a day. Silica dust and fiberglass dust exposure can also lead to COPD, with the risk unrelated to that for silicosis. The negative effects of dust exposure and cigarette smoke exposure appear to be additive or possibly more than additive.
Genetics
Genetics play a role in the development of COPD. It is more common among relatives of those with COPD who smoke than unrelated smokers. Currently, the only clearly inherited risk factor is alpha 1-antitrypsin deficiency (AAT). This risk is particularly high if someone deficient in alpha 1-antitrypsin also smokes. It is responsible for about 1–5% of cases and the condition is present in about three to four in 10,000 people. Other genetic factors are being investigated, of which many are likely.
Other
A number of other factors are less closely linked to COPD. The risk is greater in those who are poor, although whether this is due to poverty itself or other risk factors associated with poverty, such as air pollution and malnutrition, is not clear. Tentative evidence indicates that those with asthma and airway hyperreactivity are at increased risk of COPD. Birth factors such as low birth weight may also play a role, as do a number of infectious diseases, including HIV/AIDS and tuberculosis. Respiratory infections such as pneumonia do not appear to increase the risk of COPD, at least in adults.
Exacerbations
An acute exacerbation (a sudden worsening of symptoms) is commonly triggered by infection or environmental pollutants, or sometimes by other factors such as improper use of medications. Infections appear to be the cause of 50 to 75% of cases, with bacteria in 30%, viruses in 23%, and both in 25%. Environmental pollutants include both poor indoor and outdoor air quality. Exposure to personal smoke and second-hand smoke increases the risk. Cold temperatures may also play a role, with exacerbations occurring more commonly in winter. Those with more severe underlying disease have more frequent exacerbations: in mild disease 1.8 per year, moderate 2 to 3 per year, and severe 3.4 per year. Those with many exacerbations have a faster rate of deterioration of their lung function. A pulmonary embolism (PE) (blood clot in the lung) can worsen symptoms in those with pre-existing COPD. Signs of a PE in COPD include pleuritic chest pain and heart failure without signs of infection.
Pathophysiology

COPD is a type of obstructive lung disease in which chronic, incompletely reversible poor airflow (airflow limitation) and inability to breathe out fully (air trapping) exist. The poor airflow is the result of breakdown of lung tissue (known as emphysema), and small airways disease known as obstructive bronchiolitis. The relative contributions of these two factors vary between people. Severe destruction of small airways can lead to the formation of large focal lung pneumatoses, known as bullae, that replace lung tissue. This form of disease is called bullous emphysema.
COPD develops as a significant and chronic inflammatory response to inhaled irritants. Chronic bacterial infections may also add to this inflammatory state. The inflammatory cells involved include neutrophil granulocytes and macrophages, two types of white blood cells. Those who smoke additionally have Tc1 lymphocyte involvement and some people with COPD have eosinophil involvement similar to that in asthma. Part of this cell response is brought on by inflammatory mediators such as chemotactic factors. Other processes involved with lung damage include oxidative stress produced by high concentrations of free radicals in tobacco smoke and released by inflammatory cells, and breakdown of the connective tissue of the lungs by proteases that are insufficiently inhibited by protease inhibitors. The destruction of the connective tissue of the lungs leads to emphysema, which then contributes to the poor airflow, and finally, poor absorption and release of respiratory gases. General muscle wasting that often occurs in COPD may be partly due to inflammatory mediators released by the lungs into the blood.

Narrowing of the airways occurs due to inflammation and scarring within them. This contributes to the inability to breathe out fully. The greatest reduction in air flow occurs when breathing out, as the pressure in the chest is compressing the airways at this time. This can result in more air from the previous breath remaining within the lungs when the next breath is started, resulting in an increase in the total volume of air in the lungs at any given time, a process called hyperinflation or air trapping. Hyperinflation from exercise is linked to shortness of breath in COPD, as breathing in is less comfortable when the lungs are already partly filled. Hyperinflation may also worsen during an exacerbation.
Some also have a degree of airway hyperresponsiveness to irritants similar to those found in asthma.
Low oxygen levels, and eventually, high carbon dioxide levels in the blood, can occur from poor gas exchange due to decreased ventilation from airway obstruction, hyperinflation, and a reduced desire to breathe. During exacerbations, airway inflammation is also increased, resulting in increased hyperinflation, reduced expiratory airflow, and worsening of gas transfer. This can also lead to insufficient ventilation, and eventually low blood oxygen levels. Low oxygen levels, if present for a prolonged period, can result in narrowing of the arteries in the lungs, while emphysema leads to breakdown of capillaries in the lungs. Both of these changes result in increased blood pressure in the pulmonary arteries, which may cause right-sided heart failure secondary to lung disease, also known as cor pulmonale.
Diagnosis

The diagnosis of COPD should be considered in anyone over the age of 35 to 40 who has shortness of breath, a chronic cough, sputum production, or frequent winter colds and a history of exposure to risk factors for the disease. Spirometry is then used to confirm the diagnosis. Screening those without symptoms is not recommended.
Spirometry
Spirometry measures the amount of airflow obstruction present and is generally carried out after the use of a bronchodilator, a medication to open up the airways. Two main components are measured to make the diagnosis, the forced expiratory volume in one second (FEV1), which is the greatest volume of air that can be breathed out in the first second of a breath, and the forced vital capacity (FVC), which is the greatest volume of air that can be breathed out in a single large breath. Normally, 75–80% of the FVC comes out in the first second and a FEV1/FVC ratio less than 70% in someone with symptoms of COPD defines a person as having the disease. Based on these measurements, spirometry would lead to over-diagnosis of COPD in the elderly. The National Institute for Health and Care Excellence criteria additionally require a FEV1 less than 80% of predicted. People with COPD also exhibit a decrease in diffusing capacity of the lung for carbon monoxide (DLCO) due to decreased surface area in the alveoli, as well as damage to the capillary bed.
Evidence for using spirometry among those without symptoms in an effort to diagnose the condition earlier is of uncertain effect, so currently is not recommended. A peak expiratory flow (the maximum speed of expiration), commonly used in asthma, is not sufficient for the diagnosis of COPD.
Severity
| Grade | Activity affected |
|---|---|
| 1 | Only strenuous activity |
| 2 | Vigorous walking |
| 3 | With normal walking |
| 4 | After a few minutes of walking |
| 5 | With changing clothing |
| Severity | FEV1 % predicted |
|---|---|
| Mild (GOLD 1) | ≥80 |
| Moderate (GOLD 2) | 50–79 |
| Severe (GOLD 3) | 30–49 |
| Very severe (GOLD 4) | <30 |
A number of methods can determine how much COPD is affecting a given individual. The modified British Medical Research Council questionnaire or the COPD assessment test (CAT) are simple questionnaires that may be used to determine the severity of symptoms. Scores on CAT range from 0–40 with the higher the score, the more severe the disease. Spirometry may help to determine the severity of airflow limitation. This is typically based on the FEV1 expressed as a percentage of the predicted "normal" for the person's age, gender, height, and weight. Both the American and European guidelines recommend partly basing treatment recommendations on the FEV1. The GOLD guidelines suggest dividing people into four categories based on symptoms assessment and airflow limitation. Weight loss and muscle weakness, as well as the presence of other diseases, should also be taken into account.
Other tests
A chest X-ray and complete blood count may be useful to exclude other conditions at the time of diagnosis. Characteristic signs on X-ray are hyperinflated lungs, a flattened diaphragm, increased retrosternal airspace, and bullae, while it can help exclude other lung diseases, such as pneumonia, pulmonary edema, or a pneumothorax. A high-resolution CT scan of the chest may show the distribution of emphysema throughout the lungs and can also be useful to exclude other lung diseases. Unless surgery is planned, however, this rarely affects management. A saber-sheath trachea deformity may also be present. An analysis of arterial blood is used to determine the need for oxygen; this is recommended in those with an FEV1 less than 35% predicted, those with a peripheral oxygen saturation less than 92%, and those with symptoms of congestive heart failure. In areas of the world where alpha-1 antitrypsin deficiency is common, people with COPD (particularly those below the age of 45 and with emphysema affecting the lower parts of the lungs) should be considered for testing.
 89" height="120" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/0/0b/COPD.JPG/134px-COPD.JPG 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/0/0b/COPD.JPG/179px-COPD.JPG 2x" data-file-width="2998" data-file-height="4019">
89" height="120" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/0/0b/COPD.JPG/134px-COPD.JPG 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/0/0b/COPD.JPG/179px-COPD.JPG 2x" data-file-width="2998" data-file-height="4019">Chest X-ray demonstrating severe COPD: Note the small heart size in comparison to the lungs.

A lateral chest X-ray of a person with emphysema: Note the barrel chest and flat diaphragm.

Lung bulla as seen on chest X-ray in a person with severe COPD

A severe case of bullous emphysema
 91" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/f/fc/Bullus_emphasemaCT.png/180px-Bullus_emphasemaCT.png 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/f/fc/Bullus_emphasemaCT.png/240px-Bullus_emphasemaCT.png 2x" data-file-width="1019" data-file-height="772">
91" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/f/fc/Bullus_emphasemaCT.png/180px-Bullus_emphasemaCT.png 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/f/fc/Bullus_emphasemaCT.png/240px-Bullus_emphasemaCT.png 2x" data-file-width="1019" data-file-height="772">Axial CT image of the lung of a person with end-stage bullous emphysema
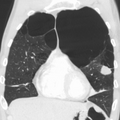
Very severe emphysema with lung cancer on the left (CT scan)
 89" height="120" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/0/0b/COPD.JPG/134px-COPD.JPG 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/0/0b/COPD.JPG/179px-COPD.JPG 2x" data-file-width="2998" data-file-height="4019">
89" height="120" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/0/0b/COPD.JPG/134px-COPD.JPG 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/0/0b/COPD.JPG/179px-COPD.JPG 2x" data-file-width="2998" data-file-height="4019">

 91" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/f/fc/Bullus_emphasemaCT.png/180px-Bullus_emphasemaCT.png 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/f/fc/Bullus_emphasemaCT.png/240px-Bullus_emphasemaCT.png 2x" data-file-width="1019" data-file-height="772">
91" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/f/fc/Bullus_emphasemaCT.png/180px-Bullus_emphasemaCT.png 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/f/fc/Bullus_emphasemaCT.png/240px-Bullus_emphasemaCT.png 2x" data-file-width="1019" data-file-height="772">
Differential diagnosis
COPD may need to be differentiated from other causes of shortness of breath such as congestive heart failure, pulmonary embolism, pneumonia, or pneumothorax. Many people with COPD mistakenly think they have asthma. The distinction between asthma and COPD is made on the basis of the symptoms, smoking history, and whether airflow limitation is reversible with bronchodilators at spirometry. Tuberculosis may also present with a chronic cough and should be considered in locations where it is common. Less common conditions that may present similarly include bronchopulmonary dysplasia and obliterative bronchiolitis. Chronic bronchitis may occur with normal airflow and in this situation it is not classified as COPD.
Prevention
Most cases of COPD are potentially preventable through decreasing exposure to smoke and improving air quality. Annual influenza vaccinations in those with COPD reduce exacerbations, hospitalizations and death. Pneumococcal vaccination may also be beneficial. Eating a diet high in beta-carotene may help but taking supplements does not seem to. A review of an oral Haemophilus influenzae vaccine found 1.6 exacerbations per year as opposed to a baseline of 2.1 in those with COPD. This small reduction was not deemed significant.
Smoking cessation
Keeping people from starting smoking is a key aspect of preventing COPD. The policies of governments, public health agencies, and antismoking organizations can reduce smoking rates by discouraging people from starting and encouraging people to stop smoking. Smoking bans in public areas and places of work are important measures to decrease exposure to secondhand smoke, and while many places have instituted bans, more are recommended.
In those who smoke, stopping smoking is the only measure shown to slow down the worsening of COPD. Even at a late stage of the disease, it can reduce the rate of worsening lung function and delay the onset of disability and death. Often, several attempts are required before long-term abstinence is achieved. Attempts over 5 years lead to success in nearly 40% of people.
Some smokers can achieve long-term smoking cessation through willpower alone. Smoking, however, is highly addictive, and many smokers need further support. The chance of quitting is improved with social support, engagement in a smoking cessation program, and the use of medications such as nicotine replacement therapy, bupropion, or varenicline. Combining smoking-cessation medication with behavioral therapy is more than twice as likely to be effective in helping people with COPD stop smoking, compared with behavioral therapy alone.
Occupational health
A number of measures have been taken to reduce the likelihood that workers in at-risk industries—such as coal mining, construction, and stonemasonry—will develop COPD. Examples of these measures include the creation of public policy, education of workers and management about the risks, promoting smoking cessation, checking workers for early signs of COPD, use of respirators, and dust control. Effective dust control can be achieved by improving ventilation, using water sprays and by using mining techniques that minimize dust generation. If a worker develops COPD, further lung damage can be reduced by avoiding ongoing dust exposure, for example by changing their work role.
Air pollution
Both indoor and outdoor air quality can be improved, which may prevent COPD or slow the worsening of existing disease. This may be achieved by public policy efforts, cultural changes, and personal involvement.
A number of developed countries have successfully improved outdoor air quality through regulations. This has resulted in improvements in the lung function of their populations. Those with COPD may experience fewer symptoms if they stay indoors on days when outdoor air quality is poor.
One key effort is to reduce exposure to smoke from cooking and heating fuels through improved ventilation of homes and better stoves and chimneys. Proper stoves may improve indoor air quality by 85%. Using alternative energy sources such as solar cooking and electrical heating is also effective. Using fuels such as kerosene or coal might be less bad than traditional biomass such as wood or dung.
Management
No cure for COPD is known, but the symptoms are treatable and its progression can be delayed. People with COPD can experience flare-ups that are often triggered by a viral or bacterial respiratory infection. The major goals of management are to reduce risk factors, manage stable COPD, prevent and treat acute exacerbations, and manage associated illnesses. The only measures that have been shown to reduce mortality are smoking cessation and supplemental oxygen. Stopping smoking decreases the risk of death by 18%. Other recommendations include influenza vaccination once a year, pneumococcal vaccination once every five years, and reduction in exposure to environmental air pollution. In those with advanced disease, palliative care may reduce symptoms, with morphine improving the feelings of shortness of breath. Noninvasive ventilation may be used to support breathing. Providing people with a personalized action plan, an educational session, and support for use of their action plan in the event of an exacerbation, reduces the number of hospital visits and encourages early treatment of exacerbations. When self-management interventions, such as taking corticosteroids and using supplemental oxygen, is combined with action plans, health-related quality of life is improved compared to usual care. Self-management is also associated with improved health-related quality of life, reduced respiratory-related and all-cause hospital admissions and improvement in shortness of breath. The 2019 NICE guidelines also recommends treatment of associated conditions.
Exercise
Pulmonary rehabilitation is a program of exercise, disease management, and counseling, coordinated to benefit the individual. In those who have had a recent exacerbation, pulmonary rehabilitation appears to improve the overall quality of life and the ability to exercise. If pulmonary rehabilitation improves mortality rates or hospital readmission rates is unclear. Pulmonary rehabilitation has been shown to improve the sense of control a person has over their disease, as well as their emotions. These programs appear to improve exercise capacity, improve health‐related quality of life, and may lower the risk of being readmitted to hospital in people recovering from an exacerbation.
The optimal exercise routine, use of noninvasive ventilation during exercise, and intensity of exercise suggested for people with COPD, is unknown. Performing endurance arm exercises improves arm movement for people with COPD, and may result in a small improvement in breathlessness. Performing arm exercises alone does not appear to improve quality of life. Breathing exercises in and of themselves appear to have a limited role. Pursed lip breathing exercises may be useful. Tai chi exercises appear to be safe to practice for people with COPD, and may be beneficial for pulmonary function and pulmonary capacity when compared to a regular treatment program. Tai Chi was not found to be more effective than other exercise intervention programs. Inspiratory and expiratory muscle training (IMT, EMT) is an effective method for improving activities of daily living (ADL). A combination of IMT and walking exercises at home may help limit breathlessness in cases of severe COPD. Additionally, the use of low amplitude high velocity joint mobilization together with exercise improves lung function and exercise capacity. The goal of spinal manipulation therapy (SMT) is to improve thoracic mobility in an effort to reduce the work on the lungs during respiration, to in turn increase exercise capacity as indicated by the results of a systemic medical review. Airway clearance techniques (ACTs), such as postural drainage, percussion/vibration, autogenic drainage, hand-held positive expiratory pressure (PEP) devices and other mechanical devices, may reduce the need for increased ventilatory assistance, the duration of ventilatory assistance, and the length of hospital stay in people with acute COPD. In people with stable COPD, ACTs may lead to short-term improvements in health-related quality of life and a reduced long-term need for hospitalisations related to respiratory issues.
Being either underweight or overweight can affect the symptoms, degree of disability, and prognosis of COPD. People with COPD who are underweight can improve their breathing muscle strength by increasing their calorie intake. When combined with regular exercise or a pulmonary rehabilitation program, this can lead to improvements in COPD symptoms. Supplemental nutrition may be useful in those who are malnourished.
Bronchodilators
Inhaled bronchodilators are the primary medications used, and result in a small overall benefit. The two major types are β2 agonists and anticholinergics; both exist in long-acting and short-acting forms. They reduce shortness of breath, wheeze, and exercise limitation, resulting in an improved quality of life. It is unclear if they change the progression of the underlying disease.
In those with mild disease, short-acting agents are recommended on an as needed basis. In those with more severe disease, long-acting agents are recommended. Long-acting agents partly work by reducing hyperinflation. If long-acting bronchodilators are insufficient, then inhaled corticosteroids are typically added. Which type of long-acting agent, long-acting muscarinic antagonist (LAMA) such as tiotropium or a long-acting beta agonist (LABA) is better is unclear, and trying each and continuing with the one that works best may be advisable. Both types of agent appear to reduce the risk of acute exacerbations by 15–25%. A 2018 review found the combination of LABA/LAMA may reduce COPD exacerbations and improve quality-of-life compared to long-acting bronchodilators alone. The 2018 NICE guideline recommends use of dual long-acting bronchodilators with economic modelling suggesting that this approach is preferable to starting one long acting bronchodilator and adding another later.
Several short-acting β2 agonists are available, including salbutamol (albuterol) and terbutaline. They provide some relief of symptoms for four to six hours. LABAs such as salmeterol, formoterol, and indacaterol are often used as maintenance therapy. Some feel the evidence of benefits is limited, while others view the evidence of benefit as established. Long-term use appears safe in COPD with adverse effects include shakiness and heart palpitations. When used with inhaled steroids they increase the risk of pneumonia. While steroids and LABAs may work better together, it is unclear if this slight benefit outweighs the increased risks. There is some evidence that combined treatment of LABAs with long-acting muscarinic antagonists (LAMA), an anticholinergic, may result in less exacerbations, less pneumonia, an improvement in forced expiratory volume (FEV1%), and potential improvements in quality of life when compared to treatment with LABA and an inhaled corticosteriod (ICS). All three together, LABA, LAMA, and ICS, have some evidence of benefits. Indacaterol requires an inhaled dose once a day, and is as effective as the other long-acting β2 agonist drugs that require twice-daily dosing for people with stable COPD.
Two main anticholinergics are used in COPD, ipratropium and tiotropium. Ipratropium is a short-acting agent, while tiotropium is long-acting. Tiotropium is associated with a decrease in exacerbations and improved quality of life, and tiotropium provides those benefits better than ipratropium. It does not appear to affect mortality or the overall hospitalization rate. Anticholinergics can cause dry mouth and urinary tract symptoms. They are also associated with increased risk of heart disease and stroke. Aclidinium, another long-acting agent, reduces hospitalizations associated with COPD and improves quality of life. The LAMA umeclidinium bromide is another anticholinergic alternative. When compared to tiotropium, the LAMAs aclidinium, glycopyrronium, and umeclidinium appear to have a similar level of efficacy; with all four being more effective than placebo. Further research is needed comparing aclidinium to tiotropium.
Corticosteroids
Corticosteroids are usually used in inhaled form, but may also be used as tablets to treat acute exacerbations. While inhaled corticosteroids (ICSs) have not shown benefit for people with mild COPD, they decrease acute exacerbations in those with either moderate or severe disease. By themselves, they have no effect on overall one-year mortality. Whether they affect the progression of the disease is unknown. When used in combination with a LABA, they may decrease mortality compared to either ICSs or LABA alone. Inhaled steroids are associated with increased rates of pneumonia. Long-term treatment with steroid tablets is associated with significant side effects.
The 2018 NICE guidelines recommend use of ICS in people with asthmatic features or features suggesting steroid responsiveness. These include any previous diagnosis of asthma or atopy, a higher blood eosinophil count, substantial variation in FEV1 over time (at least 400 mL) and at least 20% diurnal variation in peak expiratory flow. “Higher” eosinophil count was chosen, rather than specifying a particular value as it is not clear what the precise threshold should be or on how many occasions or over what time period it should be elevated.
Other medications
Long-term antibiotics, specifically those from the macrolide class such as erythromycin, reduce the frequency of exacerbations in those who have two or more a year. This practice may be cost effective in some areas of the world. Concerns include the potential for antibiotic resistance and side effects including hearing loss, tinnitus, and changes to the heart rhythm (long QT syndrome). Methylxanthines such as theophylline generally cause more harm than benefit and thus are usually not recommended, but may be used as a second-line agent in those not controlled by other measures. Mucolytics may help to reduce exacerbations in some people with chronic bronchitis; noticed by less hospitalization and less days of disability in one month. Cough medicines are not recommended.
For people with COPD, the use of cardioselective (heart-specific) beta-blocker therapy does not appear to impair respiratory function. Cardioselective beta-blocker therapy should not be contraindicated for people with COPD. In those with low levels of vitamin D, supplementation reduces the risk of exacerbations.
Oxygen
Supplemental oxygen is recommended in those with low oxygen levels at rest (a partial pressure of oxygen less than 50–55 mmHg or oxygen saturations of less than 88%). In this group of people, it decreases the risk of heart failure and death if used 15 hours per day and may improve people's ability to exercise. In those with normal or mildly low oxygen levels, oxygen supplementation may improve shortness of breath when given during exercise, but may not improve breathlessness during normal daily activities or affect the quality of life. A risk of fires and little benefit exist when those on oxygen continue to smoke. In this situation, some (including NICE) recommend against its use. During acute exacerbations, many require oxygen therapy; the use of high concentrations of oxygen without taking into account a person's oxygen saturations may lead to increased levels of carbon dioxide and worsened outcomes. In those at high risk of high carbon dioxide levels, oxygen saturations of 88–92% are recommended, while for those without this risk, recommended levels are 94–98%.
Surgery
For those with very severe disease, surgery is sometimes helpful and may include lung transplantation or lung volume-reduction surgery, which involves removing the parts of the lung most damaged by emphysema, allowing the remaining, relatively good lung to expand and work better. It seems to be particularly effective if emphysema predominantly involves the upper lobe, but the procedure increases the risks of adverse events and early death for people who have diffuse emphysema. The procedure also increases the risk of adverse effects for people with moderate to severe COPD. Lung transplantation is sometimes performed for very severe COPD, particularly in younger individuals