Hiv/aids

Human immunodeficiency virus infection and acquired immunodeficiency syndrome (HIV/AIDS) is a spectrum of conditions caused by infection with the human immunodeficiency virus (HIV), a retrovirus. Following initial infection a person may not notice any symptoms, or may experience a brief period of influenza-like illness. Typically, this is followed by a prolonged period with no symptoms. If the infection progresses, it interferes more with the immune system, increasing the risk of developing common infections such as tuberculosis, as well as other opportunistic infections, and tumors which are otherwise rare in people who have normal immune function. These late symptoms of infection are referred to as acquired immunodeficiency syndrome (AIDS). This stage is often also associated with unintended weight loss.
HIV is spread primarily by unprotected sex (including anal and oral sex), contaminated blood transfusions, hypodermic needles, and from mother to child during pregnancy, delivery, or breastfeeding. Some bodily fluids, such as saliva, sweat and tears, do not transmit the virus.
Methods of prevention include safe sex, needle exchange programs, treating those who are infected, and pre- & post-exposure prophylaxis. Disease in a baby can often be prevented by giving both the mother and child antiretroviral medication. There is no cure or vaccine; however, antiretroviral treatment can slow the course of the disease and may lead to a near-normal life expectancy. Treatment is recommended as soon as the diagnosis is made. Without treatment, the average survival time after infection is 11 years.
In 2018, about 37.9 million people were living with HIV and it resulted in 770,000 deaths. An estimated 20.6 million of these live in eastern and southern Africa. Between the time that AIDS was identified (in the early 1980s) and 2018, the disease caused an estimated 32 million deaths worldwide. HIV/AIDS is considered a pandemic—a disease outbreak which is present over a large area and is actively spreading.
HIV made the jump from other primates to humans in west-central Africa in the early-to-mid 20th century. AIDS was first recognized by the United States Centers for Disease Control and Prevention (CDC) in 1981 and its cause—HIV infection—was identified in the early part of the decade.
HIV/AIDS has had a large impact on society, both as an illness and as a source of discrimination. The disease also has large economic impacts. There are many misconceptions about HIV/AIDS, such as the belief that it can be transmitted by casual non-sexual contact. The disease has become subject to many controversies involving religion, including the Catholic Church's position not to support condom use as prevention. It has attracted international medical and political attention as well as large-scale funding since it was identified in the 1980s.
 Play media
Play mediaSigns and symptoms
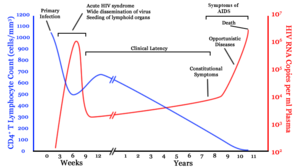
There are three main stages of HIV infection: acute infection, clinical latency, and AIDS.
Acute infection
 1/1b/Symptoms_of_acute_HIV_infection.svg/280px-Symptoms_of_acute_HIV_infection.svg.png" decoding="async" width="280" height="250" class="thumbimage" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/1/1b/Symptoms_of_acute_HIV_infection.svg/420px-Symptoms_of_acute_HIV_infection.svg.png 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/1/1b/Symptoms_of_acute_HIV_infection.svg/560px-Symptoms_of_acute_HIV_infection.svg.png 2x" data-file-width="1133" data-file-height="1012">
1/1b/Symptoms_of_acute_HIV_infection.svg/280px-Symptoms_of_acute_HIV_infection.svg.png" decoding="async" width="280" height="250" class="thumbimage" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/1/1b/Symptoms_of_acute_HIV_infection.svg/420px-Symptoms_of_acute_HIV_infection.svg.png 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/1/1b/Symptoms_of_acute_HIV_infection.svg/560px-Symptoms_of_acute_HIV_infection.svg.png 2x" data-file-width="1133" data-file-height="1012"> The initial period following the contraction of HIV is called acute HIV, primary HIV or acute retroviral syndrome. Many individuals develop an influenza-like illness or a mononucleosis-like illness 2–4 weeks after exposure while others have no significant symptoms. Symptoms occur in 40–90% of cases and most commonly include fever, large tender lymph nodes, throat inflammation, a rash, headache, tiredness, and/or sores of the mouth and genitals. The rash, which occurs in 20–50% of cases, presents itself on the trunk and is maculopapular, classically. Some people also develop opportunistic infections at this stage. Gastrointestinal symptoms, such as vomiting or diarrhea may occur. Neurological symptoms of peripheral neuropathy or Guillain–Barré syndrome also occurs. The duration of the symptoms varies, but is usually one or two weeks.
Owing to their nonspecific character, these symptoms are not often recognized as signs of HIV infection. Even cases that do get seen by a family doctor or a hospital are often misdiagnosed as one of the many common infectious diseases with overlapping symptoms. Thus, it is recommended that HIV be considered in people presenting with an unexplained fever who may have risk factors for the infection.
Clinical latency
The initial symptoms are followed by a stage called clinical latency, asymptomatic HIV, or chronic HIV. Without treatment, this second stage of the natural history of HIV infection can last from about three years to over 20 years (on average, about eight years). While typically there are few or no symptoms at first, near the end of this stage many people experience fever, weight loss, gastrointestinal problems and muscle pains. Between 50% and 70% of people also develop persistent generalized lymphadenopathy, characterized by unexplained, non-painful enlargement of more than one group of lymph nodes (other than in the groin) for over three to six months.
Although most HIV-1 infected individuals have a detectable viral load and in the absence of treatment will eventually progress to AIDS, a small proportion (about 5%) retain high levels of CD4+ T cells (T helper cells) without antiretroviral therapy for more than five years. These individuals are classified as "HIV controllers" or long-term nonprogressors (LTNP). Another group consists of those who maintain a low or undetectable viral load without anti-retroviral treatment, known as "elite controllers" or "elite suppressors". They represent approximately 1 in 300 infected persons.
Acquired immunodeficiency syndrome

Acquired immunodeficiency syndrome (AIDS) is defined as an HIV infection with either a CD4+ T cell count below 200 cells per µL or the occurrence of specific diseases associated with HIV infection. In the absence of specific treatment, around half of people infected with HIV develop AIDS within ten years. The most common initial conditions that alert to the presence of AIDS are pneumocystis pneumonia (40%), cachexia in the form of HIV wasting syndrome (20%), and esophageal candidiasis. Other common signs include recurrent respiratory tract infections.
Opportunistic infections may be caused by bacteria, viruses, fungi, and parasites that are normally controlled by the immune system. Which infections occur depends partly on what organisms are common in the person's environment. These infections may affect nearly every organ system.
People with AIDS have an increased risk of developing various viral-induced cancers, including Kaposi's sarcoma, Burkitt's lymphoma, primary central nervous system lymphoma, and cervical cancer. Kaposi's sarcoma is the most common cancer, occurring in 10% to 20% of people with HIV. The second-most common cancer is lymphoma, which is the cause of death of nearly 16% of people with AIDS and is the initial sign of AIDS in 3% to 4%. Both these cancers are associated with human herpesvirus 8 (HHV-8). Cervical cancer occurs more frequently in those with AIDS because of its association with human papillomavirus (HPV). Conjunctival cancer (of the layer that lines the inner part of eyelids and the white part of the eye) is also more common in those with HIV.
Additionally, people with AIDS frequently have systemic symptoms such as prolonged fevers, sweats (particularly at night), swollen lymph nodes, chills, weakness, and unintended weight loss. Diarrhea is another common symptom, present in about 90% of people with AIDS. They can also be affected by diverse psychiatric and neurological symptoms independent of opportunistic infections and cancers.
Transmission
| Exposure route | Chance of infection | |||
|---|---|---|---|---|
| Blood transfusion | 90% | |||
| Childbirth (to child) | 25% | |||
| Needle-sharing injection drug use | 0.67% | |||
| Percutaneous needle stick | 0.30% | |||
| Receptive anal intercourse* | 0.04–3.0% | |||
| Insertive anal intercourse* | 0.03% | |||
| Receptive penile-vaginal intercourse* | 0.05–0.30% | |||
| Insertive penile-vaginal intercourse* | 0.01–0.38% | |||
| Receptive oral intercourse*§ | 0–0.04% | |||
| Insertive oral intercourse*§ | 0–0.005% | |||
| * assuming no condom use § source refers to oral intercourse performed on a man | ||||
HIV is spread by three main routes: sexual contact, significant exposure to infected body fluids or tissues, and from mother to child during pregnancy, delivery, or breastfeeding (known as vertical transmission). There is no risk of acquiring HIV if exposed to feces, nasal secretions, saliva, sputum, sweat, tears, urine, or vomit unless these are contaminated with blood. It is also possible to be co-infected by more than one strain of HIV—a condition known as HIV superinfection.
Sexual
The most frequent mode of transmission of HIV is through sexual contact with an infected person. However, an HIV-positive person who has an undetectable viral load as a result of long-term treatment has effectively no risk of transmitting HIV sexually. The existence of functionally noncontagious HIV-positive people on antiretroviral therapy was controversially publicized in the 2008 Swiss Statement, and has since become accepted as medically sound.
Globally, the most common mode of HIV transmission is via sexual contacts between people of the opposite sex; however, the pattern of transmission varies among countries. As of 2017[update], most HIV transmission in the United States occurred among men who had sex with men (82% of new HIV diagnoses among males aged 13 and older and 70% of total new diagnoses). In the US, gay and bisexual men aged 13 to 24 accounted for an estimated 92% of new HIV diagnoses among all men in their age group and 27% of new diagnoses among all gay and bisexual men.
With regard to unprotected heterosexual contacts, estimates of the risk of HIV transmission per sexual act appear to be four to ten times higher in low-income countries than in high-income countries. In low-income countries, the risk of female-to-male transmission is estimated as 0.38% per act, and of male-to-female transmission as 0.30% per act; the equivalent estimates for high-income countries are 0.04% per act for female-to-male transmission, and 0.08% per act for male-to-female transmission. The risk of transmission from anal intercourse is especially high, estimated as 1.4–1.7% per act in both heterosexual and homosexual contacts. While the risk of transmission from oral sex is relatively low, it is still present. The risk from receiving oral sex has been described as "nearly nil"; however, a few cases have been reported. The per-act risk is estimated at 0–0.04% for receptive oral intercourse. In settings involving prostitution in low-income countries, risk of female-to-male transmission has been estimated as 2.4% per act, and of male-to-female transmission as 0.05% per act.
Risk of transmission increases in the presence of many sexually transmitted infections and genital ulcers. Genital ulcers appear to increase the risk approximately fivefold. Other sexually transmitted infections, such as gonorrhea, chlamydia, trichomoniasis, and bacterial vaginosis, are associated with somewhat smaller increases in risk of transmission.
The viral load of an infected person is an important risk factor in both sexual and mother-to-child transmission. During the first 2.5 months of an HIV infection a person's infectiousness is twelve times higher due to the high viral load associated with acute HIV. If the person is in the late stages of infection, rates of transmission are approximately eightfold greater.
Commercial sex workers (including those in pornography) have an increased likelihood of contracting HIV. Rough sex can be a factor associated with an increased risk of transmission. Sexual assault is also believed to carry an increased risk of HIV transmission as condoms are rarely worn, physical trauma to the vagina or rectum is likely, and there may be a greater risk of concurrent sexually transmitted infections.
Body fluids

The second-most frequent mode of HIV transmission is via blood and blood products. Blood-borne transmission can be through needle-sharing during intravenous drug use, needle-stick injury, transfusion of contaminated blood or blood product, or medical injections with unsterilized equipment. The risk from sharing a needle during drug injection is between 0.63% and 2.4% per act, with an average of 0.8%. The risk of acquiring HIV from a needle stick from an HIV-infected person is estimated as 0.3% (about 1 in 333) per act and the risk following mucous membrane exposure to infected blood as 0.09% (about 1 in 1000) per act. This risk may, however, be up to 5% if the introduced blood was from a person with a high viral load and the cut was deep. In the United States intravenous drug users made up 12% of all new cases of HIV in 2009, and in some areas more than 80% of people who inject drugs are HIV-positive.
HIV is transmitted in about 90% of blood transfusions using infected blood. In developed countries the risk of acquiring HIV from a blood transfusion is extremely low (less than one in half a million) where improved donor selection and HIV screening is performed; for example, in the UK the risk is reported at one in five million and in the United States it was one in 1.5 million in 2008. In low-income countries, only half of transfusions may be appropriately screened (as of 2008), and it is estimated that up to 15% of HIV infections in these areas come from transfusion of infected blood and blood products, representing between 5% and 10% of global infections. It is possible to acquire HIV from organ and tissue transplantation, although this is rare because of screening.
Unsafe medical injections play a role in HIV spread in sub-Saharan Africa. In 2007, between 12% and 17% of infections in this region were attributed to medical syringe use. The World Health Organization estimates the risk of transmission as a result of a medical injection in Africa at 1.2%. Risks are also associated with invasive procedures, assisted delivery, and dental care in this area of the world.
People giving or receiving tattoos, piercings, and scarification are theoretically at risk of infection but no confirmed cases have been documented. It is not possible for mosquitoes or other insects to transmit HIV.
Mother-to-child
HIV can be transmitted from mother to child during pregnancy, during delivery, or through breast milk, resulting in the baby also contracting HIV. As of 2008, vertical transmission accounted for about 90% of cases of HIV in children. In the absence of treatment, the risk of transmission before or during birth is around 20%, and in those who also breastfeed 35%. Treatment decreases this risk to less than 5%.
Antiretrovirals when taken by either the mother or the baby decrease the risk of transmission in those who do breastfeed. If blood contaminates food during pre-chewing it may pose a risk of transmission. If a woman is untreated, two years of breastfeeding results in an HIV/AIDS risk in her baby of about 17%. Due to the increased risk of death without breastfeeding in many areas in the developing world, the World Health Organization recommends either exclusive breastfeeding or the provision of safe formula. All women known to be HIV-positive should be taking lifelong antiretroviral therapy.
Virology
 1/1a/HIV-budding-Color.jpg/220px-HIV-budding-Color.jpg" decoding="async" width="220" height="146" class="thumbimage" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/1/1a/HIV-budding-Color.jpg/330px-HIV-budding-Color.jpg 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/1/1a/HIV-budding-Color.jpg/440px-HIV-budding-Color.jpg 2x" data-file-width="2967" data-file-height="1971">
1/1a/HIV-budding-Color.jpg/220px-HIV-budding-Color.jpg" decoding="async" width="220" height="146" class="thumbimage" srcset="//upload.wikimedia.org/wikipedia/commons/thumb/1/1a/HIV-budding-Color.jpg/330px-HIV-budding-Color.jpg 1.5x, //upload.wikimedia.org/wikipedia/commons/thumb/1/1a/HIV-budding-Color.jpg/440px-HIV-budding-Color.jpg 2x" data-file-width="2967" data-file-height="1971"> HIV is the cause of the spectrum of disease known as HIV/AIDS. HIV is a retrovirus that primarily infects components of the human immune system such as CD4+ T cells, macrophages and dendritic cells. It directly and indirectly destroys CD4+ T cells.
HIV is a member of the genus Lentivirus, part of the family Retroviridae. Lentiviruses share many morphological and biological characteristics. Many species of mammals are infected by lentiviruses, which are characteristically responsible for long-duration illnesses with a long incubation period. Lentiviruses are transmitted as single-stranded, positive-sense, enveloped RNA viruses. Upon entry into the target cell, the viral RNA genome is converted (reverse transcribed) into double-stranded DNA by a virally encoded reverse transcriptase that is transported along with the viral genome in the virus particle. The resulting viral DNA is then imported into the cell nucleus and integrated into the cellular DNA by a virally encoded integrase and host co-factors. Once integrated, the virus may become latent, allowing the virus and its host cell to avoid detection by the immune system. Alternatively, the virus may be transcribed, producing new RNA genomes and viral proteins that are packaged and released from the cell as new virus particles that begin the replication cycle anew.
HIV is now known to spread between CD4+ T cells by two parallel routes: cell-free spread and cell-to-cell spread, i.e. it employs hybrid spreading mechanisms. In the cell-free spread, virus particles bud from an infected T cell, enter the blood/extracellular fluid and then infect another T cell following a chance encounter. HIV can also disseminate by direct transmission from one cell to another by a process of cell-to-cell spread. The hybrid spreading mechanisms of HIV contribute to the virus's ongoing replication against antiretroviral therapies.
Two types of HIV have been characterized: HIV-1 and HIV-2. HIV-1 is the virus that was originally discovered (and initially referred to also as LAV or HTLV-III). It is more virulent, more infective, and is the cause of the majority of HIV infections globally. The lower infectivity of HIV-2 as compared with HIV-1 implies that fewer people exposed to HIV-2 will be infected per exposure. Because of its relatively poor capacity for transmission, HIV-2 is largely confined to West Africa.
Pathophysiology
 Play media
Play media
After the virus enters the body there is a period of rapid viral replication, leading to an abundance of virus in the peripheral blood. During primary infection, the level of HIV may reach several million virus particles per milliliter of blood. This response is accompanied by a marked drop in the number of circulating CD4+ T cells. The acute viremia is almost invariably associated with activation of CD8+ T cells, which kill HIV-infected cells, and subsequently with antibody production, or seroconversion. The CD8+ T cell response is thought to be important in controlling virus levels, which peak and then decline, as the CD4+ T cell counts recover. A good CD8+ T cell response has been linked to slower disease progression and a better prognosis, though it does not eliminate the virus.
Ultimately, HIV causes AIDS by depleting CD4+ T cells. This weakens the immune system and allows opportunistic infections. T cells are essential to the immune response and without them, the body cannot fight infections or kill cancerous cells. The mechanism of CD4+ T cell depletion differs in the acute and chronic phases. During the acute phase, HIV-induced cell lysis and killing of infected cells by CD8+ T cells accounts for CD4+ T cell depletion, although apoptosis may also be a factor. During the chronic phase, the consequences of generalized immune activation coupled with the gradual loss of the ability of the immune system to generate new T cells appear to account for the slow decline in CD4+ T cell numbers.
Although the symptoms of immune deficiency characteristic of AIDS do not appear for years after a person is infected, the bulk of CD4+ T cell loss occurs during the first weeks of infection, especially in the intestinal mucosa, which harbors the majority of the lymphocytes found in the body. The reason for the preferential loss of mucosal CD4+ T cells is that the majority of mucosal CD4+ T cells express the CCR5 protein which HIV uses as a co-receptor to gain access to the cells, whereas only a small fraction of CD4+ T cells in the bloodstream do so. A specific genetic change that alters the CCR5 protein when present in both chromosomes very effectively prevents HIV-1 infection.
HIV seeks out and destroys CCR5 expressing CD4+ T cells during acute infection. A vigorous immune response eventually controls the infection and initiates the clinically latent phase. CD4+ T cells in mucosal tissues remain particularly affected. Continuous HIV replication causes a state of generalized immune activation persisting throughout the chronic phase. Immune activation, which is reflected by the increased activation state of immune cells and release of pro-inflammatory cytokines, results from the activity of several HIV gene products and the immune response to ongoing HIV replication. It is also linked to the breakdown of the immune surveillance system of the gastrointestinal mucosal barrier caused by the depletion of mucosal CD4+ T cells during the acute phase of disease.
Diagnosis
| Blood test | Days |
|---|---|
| Antibody test (rapid test, ELISA 3rd gen) | 23–90 |
| Antibody and p24 antigen test (ELISA 4th gen) | 18–45 |
| PCR | 10–33 |
HIV/AIDS is diagnosed via laboratory testing and then staged based on the presence of certain signs or symptoms. HIV screening is recommended by the United States Preventive Services Task Force for all people 15 years to 65 years of age, including all pregnant women. Additionally, testing is recommended for those at high risk, which includes anyone diagnosed with a sexually transmitted illness. In many areas of the world, a third of HIV carriers only discover they are infected at an advanced stage of the disease when AIDS or severe immunodeficiency has become apparent.
HIV testing


Most people infected with HIV develop specific antibodies (i.e. seroconvert) within three to twelve weeks after the initial infection. Diagnosis of primary HIV before seroconversion is done by measuring HIV-RNA or p24 antigen. Positive results obtained by antibody or PCR testing are confirmed either by a different antibody or by PCR.
Antibody tests in children younger than 18 months are typically inaccurate, due to the continued presence of maternal antibodies. Thus HIV infection can only be diagnosed by PCR testing for HIV RNA or DNA, or via testing for the p24 antigen. Much of the world lacks access to reliable PCR testing, and people in many places simply wait until either symptoms develop or the child is old enough for accurate antibody testing. In sub-Saharan Africa between 2007 and 2009, between 30% and 70% of the population were aware of their HIV status. In 2009, between 3.6% and 42% of men and women in sub-Saharan countries were tested; this represented a significant increase compared to previous years.
Classifications
Two main clinical staging systems are used to classify HIV and HIV-related disease for surveillance purposes: the WHO disease staging system for HIV infection and disease, and the CDC classification system for HIV infection. The CDC's classification system is more frequently adopted in developed countries. Since the WHO's staging system does not require laboratory tests, it is suited to the resource-restricted conditions encountered in developing countries, where it can also be used to help guide clinical management. Despite their differences, the two systems allow comparison for statistical purposes.
The World Health Organization first proposed a definition for AIDS in 1986. Since then, the WHO classification has been updated and expanded several times, with the most recent version being published in 2007. The WHO system uses the following categories:
- Primary HIV infection: May be either asymptomatic or associated with acute retroviral syndrome
- Stage I: HIV infection is asymptomatic with a CD4+ T cell count (also known as CD4 count) greater than 500 per microlitre (µl or cubic mm) of blood. May include generalized lymph node enlargement.
- Stage II: Mild symptoms, which may include minor mucocutaneous manifestations and recurrent upper respiratory tract infections. A CD4 count of less than 500/µl
- Stage III: Advanced symptoms, which may include unexplained chronic diarrhea for longer than a month, severe bacterial infections including tuberculosis of the lung, and a CD4 count of less than 350/µl
- Stage IV or AIDS: severe symptoms, which include toxoplasmosis of the brain, candidiasis of the esophagus, trachea, bronchi, or lungs, and Kaposi's sarcoma. A CD4 count of less than 200/µl
The United States Center for Disease Control and Prevention also created a classification system for HIV, and updated it in 2008 and 2014. This system classifies HIV infections based on CD4 count and clinical symptoms, and describes the infection in five groups. In those greater than six years of age it is:
- Stage 0: the time between a negative or indeterminate HIV test followed less than 180 days by a positive test.
- Stage 1: CD4 count ≥ 500 cells/µl and no AIDS-defining conditions.
- Stage 2: CD4 count 200 to 500 cells/µl and no AIDS-defining conditions.
- Stage 3: CD4 count ≤ 200 cells/µl or AIDS-defining conditions.
- Unknown: if insufficient information is available to make any of the above classifications.
For surveillance purposes, the AIDS diagnosis still stands even if, after treatment, the CD4+ T cell count rises to above 200 per µL of blood or other AIDS-defining illnesses are cured.
Prevention

Sexual contact

Consistent condom use reduces the risk of HIV transmission by approximately 80% over the long term. When condoms are used consistently by a couple in which one person is infected, the rate of HIV infection is less than 1% per year. There is some evidence to suggest that female condoms may provide an equivalent level of protection. Application of a vaginal gel containing tenofovir (a reverse transcriptase inhibitor) immediately before sex seems to reduce infection rates by approximately 40% among African women. By contrast, use of the spermicide nonoxynol-9 may increase the risk of transmission due to its tendency to cause vaginal and rectal irritation.
Circumcision in Sub-Saharan Africa "reduces the acquisition of HIV by heterosexual men by between 38% and 66% over 24 months". Owing to these studies, both the World Health Organization and UNAIDS recommended male circumcision in 2007 as a method of preventing female-to-male HIV transmission in areas with high rates of HIV. However, whether